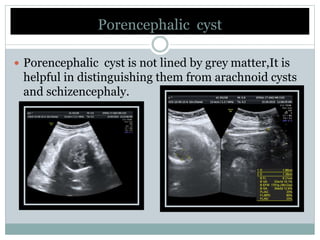
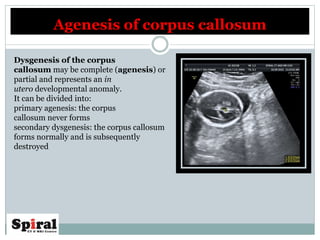
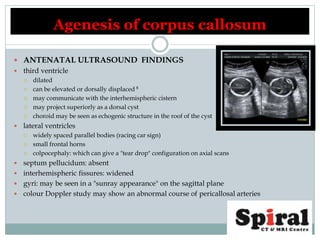
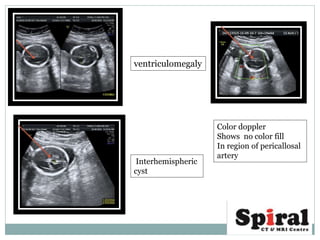
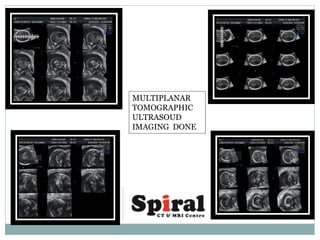
The document discusses various congenital disorders, including porencephaly, muscle hernias, septo-optic dysplasia, and agenesis of the corpus callosum, providing definitions, etiology, clinical presentations, and diagnostic methods. It highlights the importance of imaging techniques like ultrasound and MRI in diagnosing conditions like porencephalic cysts and muscle hernias, as well as the factors contributing to fetal malformations. Additionally, it outlines the characteristic features and associated risks of these congenital anomalies, emphasizing genetic counseling where necessary.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









