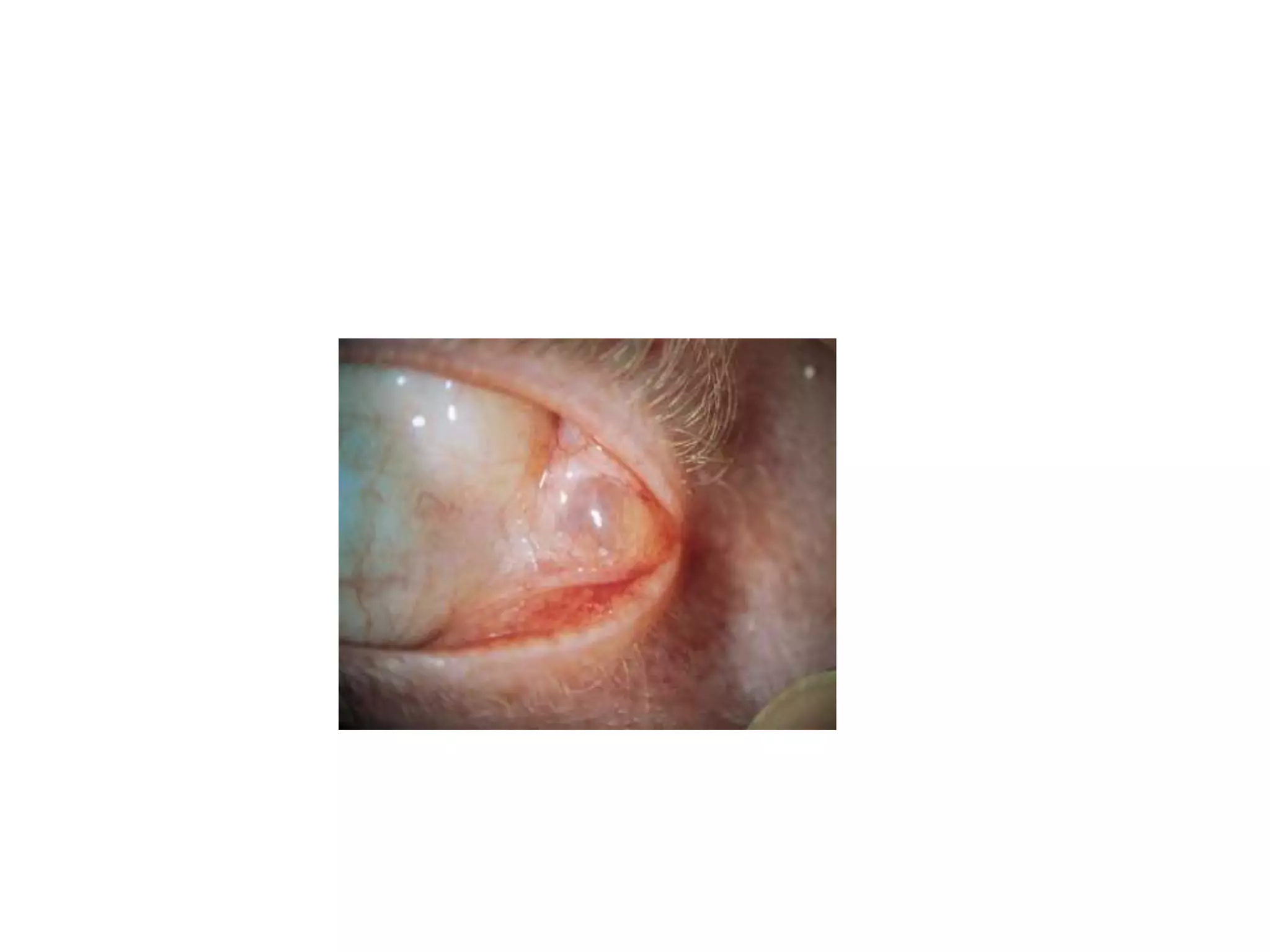
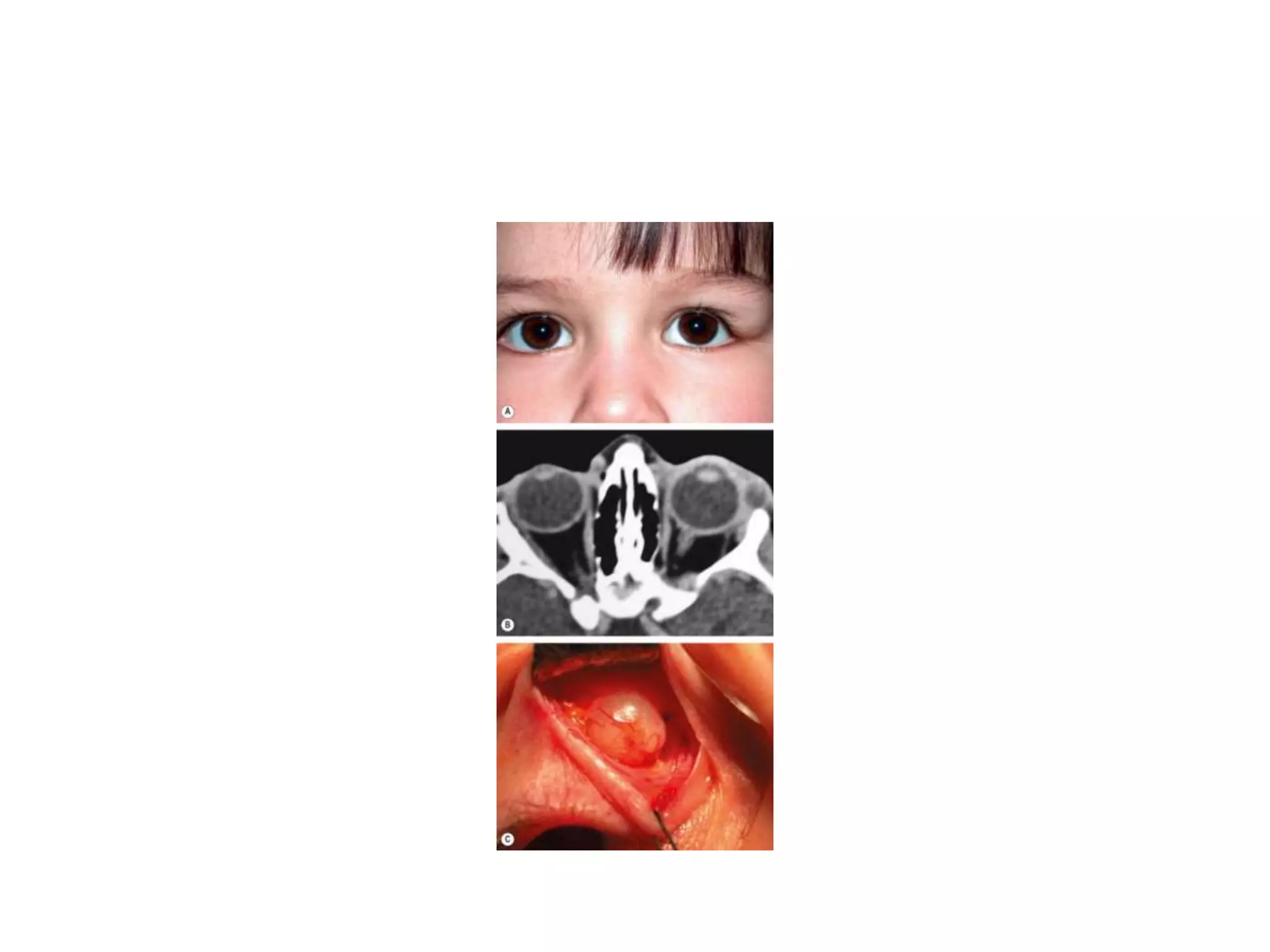
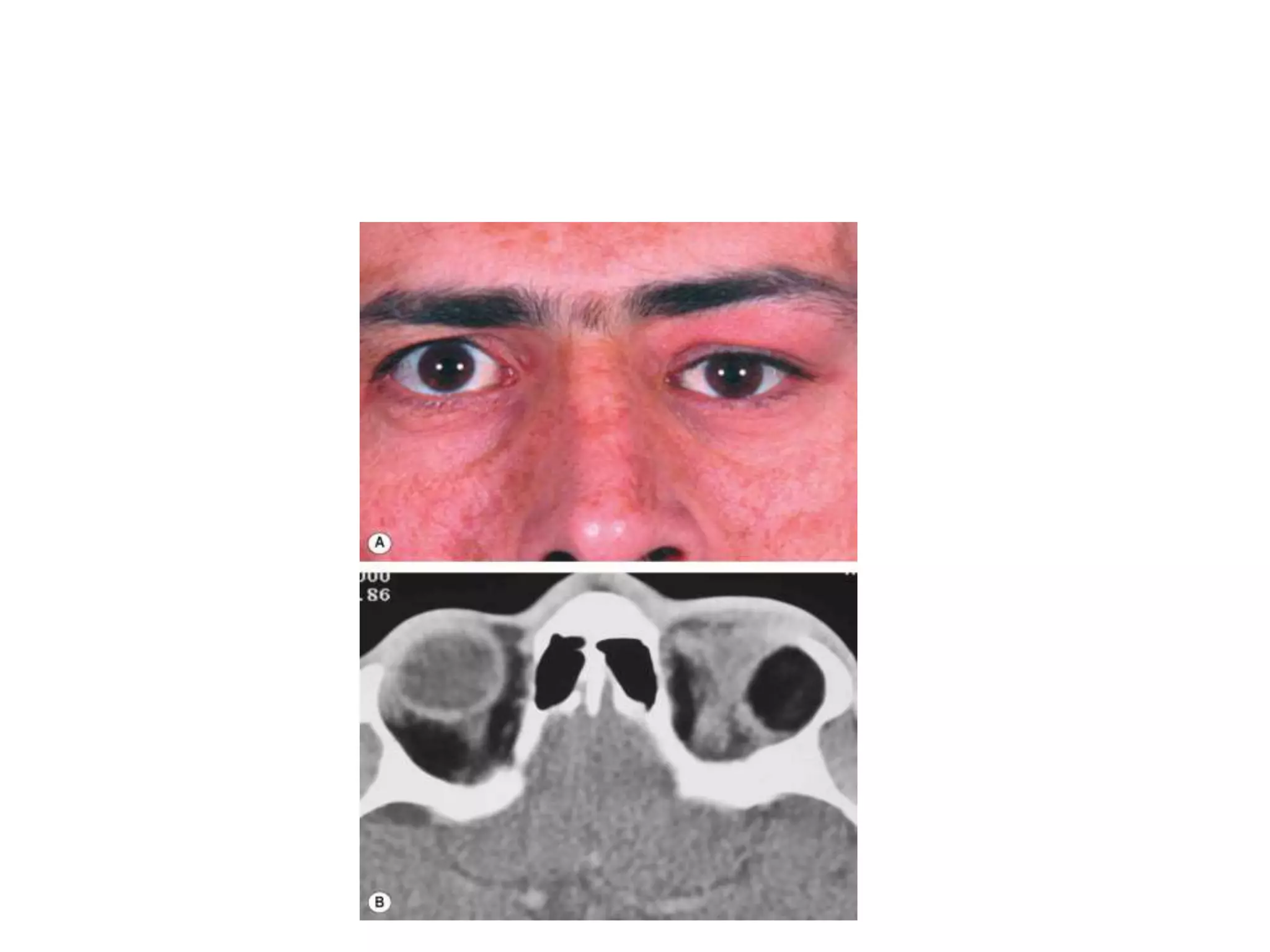
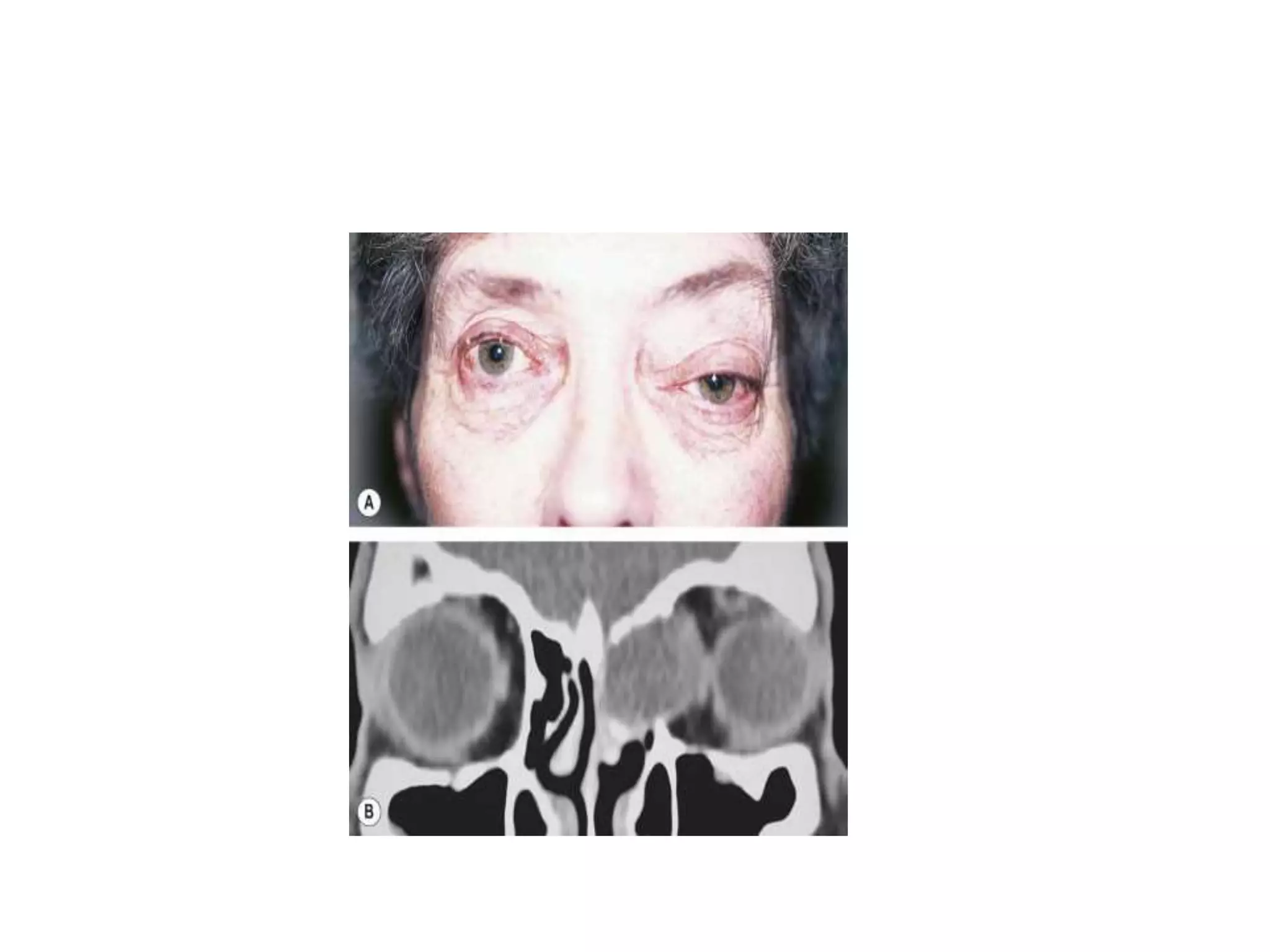
This document discusses several types of cystic lesions that can occur in the orbit, including dacryops, dermoid cysts, sinus mucoceles, and encephaloceles. Dacryops are cysts of the lacrimal gland that present as round protrusions in the upper eyelid. Dermoid cysts are lined with skin and contain skin structures, and can be superficial or deep. Sinus mucoceles occur when sinus drainage is obstructed, causing a mucus-filled cyst. Encephaloceles are herniations of brain or meninges through skull defects that can displace the eyeball.











































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










