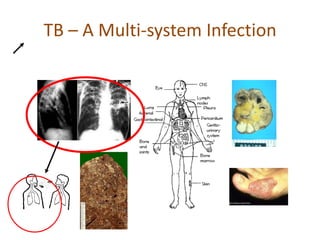
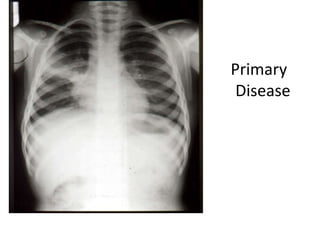
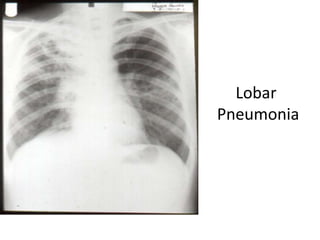
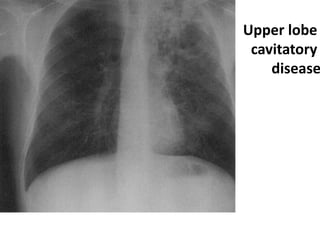
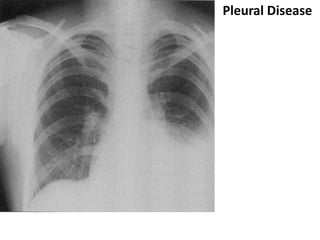
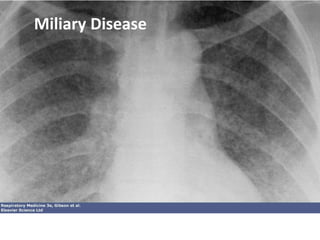
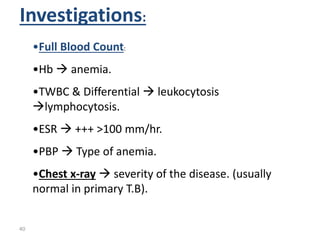
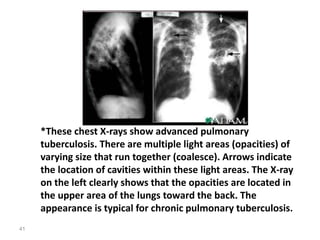
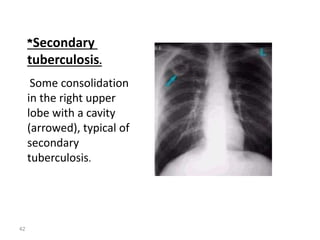
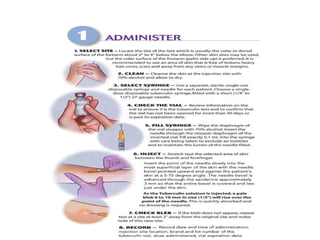
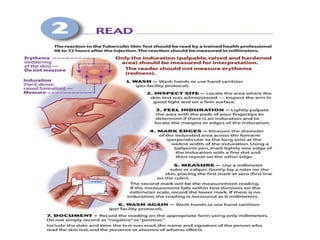
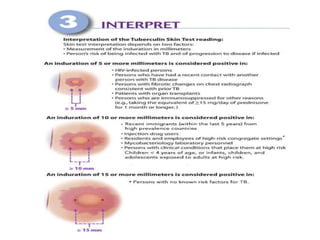
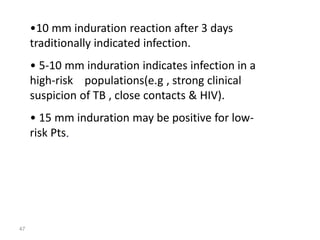
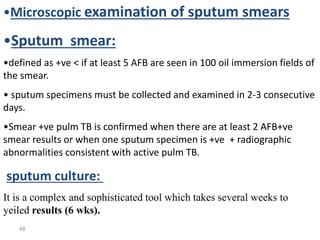
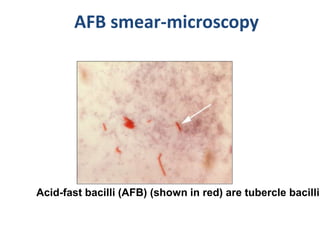
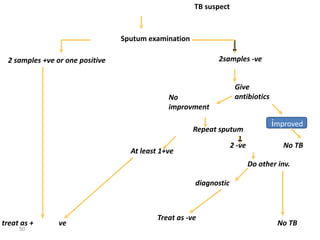
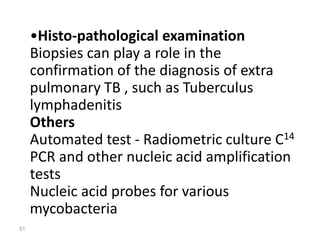
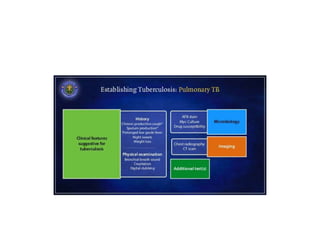
Tuberculosis is a chronic infectious disease caused by the bacterium Mycobacterium tuberculosis. It typically affects the lungs but can also affect other parts of the body. It spreads through the air when people who are sick with TB disease of the lungs or throat cough, sneeze, speak, or sing. Diagnosis involves a combination of physical examination, chest X-ray, tuberculin skin test, blood tests, and microbiological examinations of body fluids and tissues. Treatment requires multiple antibiotics taken for a minimum of 6 months. Proper treatment is important to cure the individual and prevent further transmission.













![TBc[1].ppt comuuintiy awwenaes in somali](https://cdn.slidesharecdn.com/ss_thumbnails/tbc1-241211101334-4fc36c41-thumbnail.jpg?width=640&height=640&fit=bounds)








































