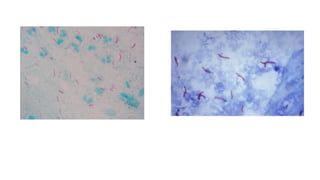
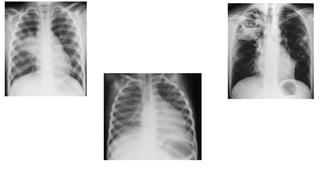
Tuberculosis (TB) is a contagious disease primarily affecting the lungs, caused by Mycobacterium tuberculosis, and characterized by symptoms such as cough, fever, and weight loss. TB can be classified into primary and secondary types, with extrapulmonary forms affecting different body parts, and is diagnosed through bacteriological tests, sputum cultures, radiography, and the tuberculin skin test. Treatment involves various therapeutic approaches tailored to the type and extent of the infection.