This document provides an update on Inova Health System's Picker Grant project to improve patient handoffs. It discusses:
1) The goals of exploring patient perceptions of bedside handoffs and promoting "Always Events" where patients are included in care transitions.
2) Background on the Picker Institute which supports patient-centered care research and the "Always Events" framework for driving systems to be more patient-focused.
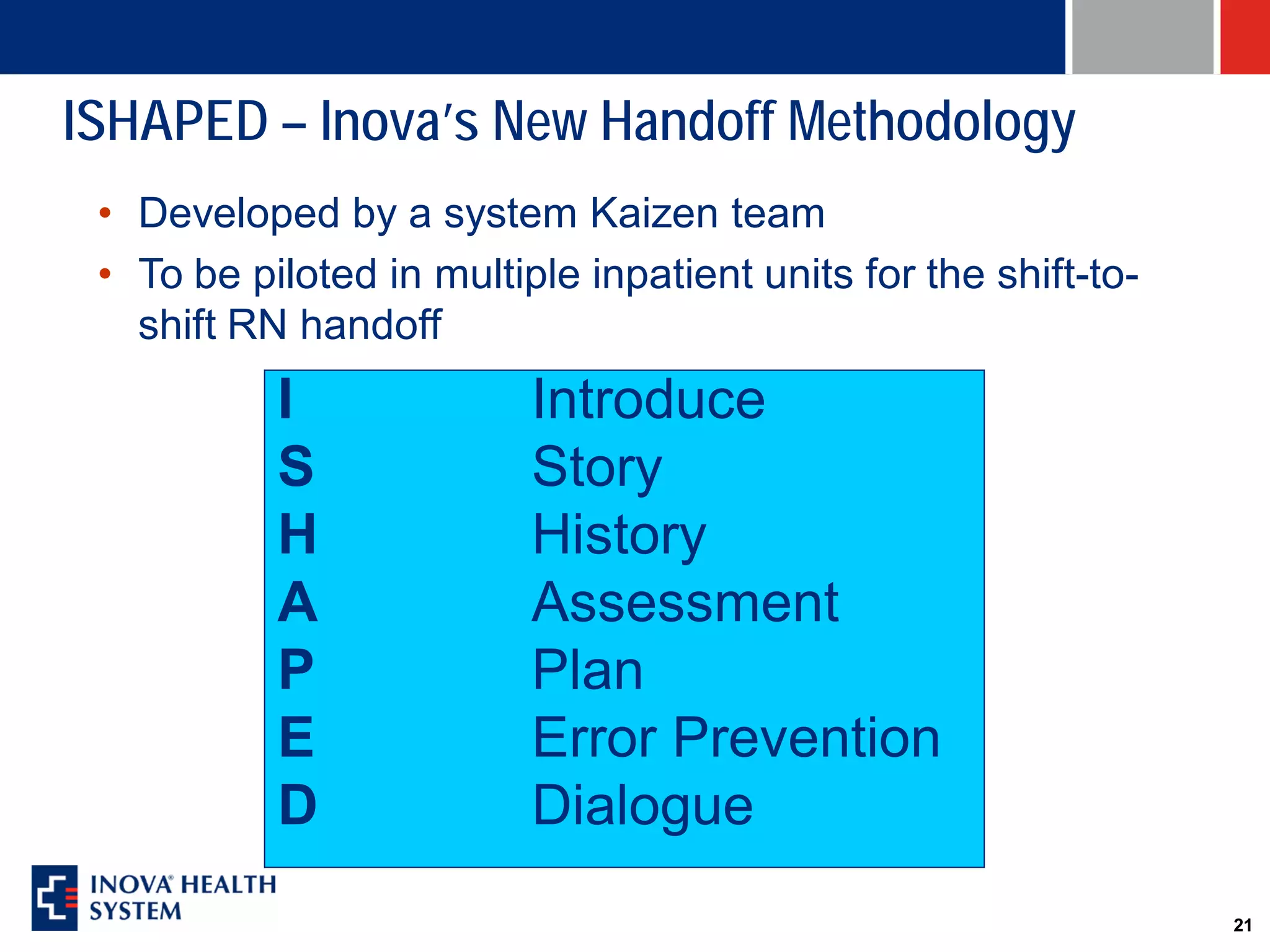
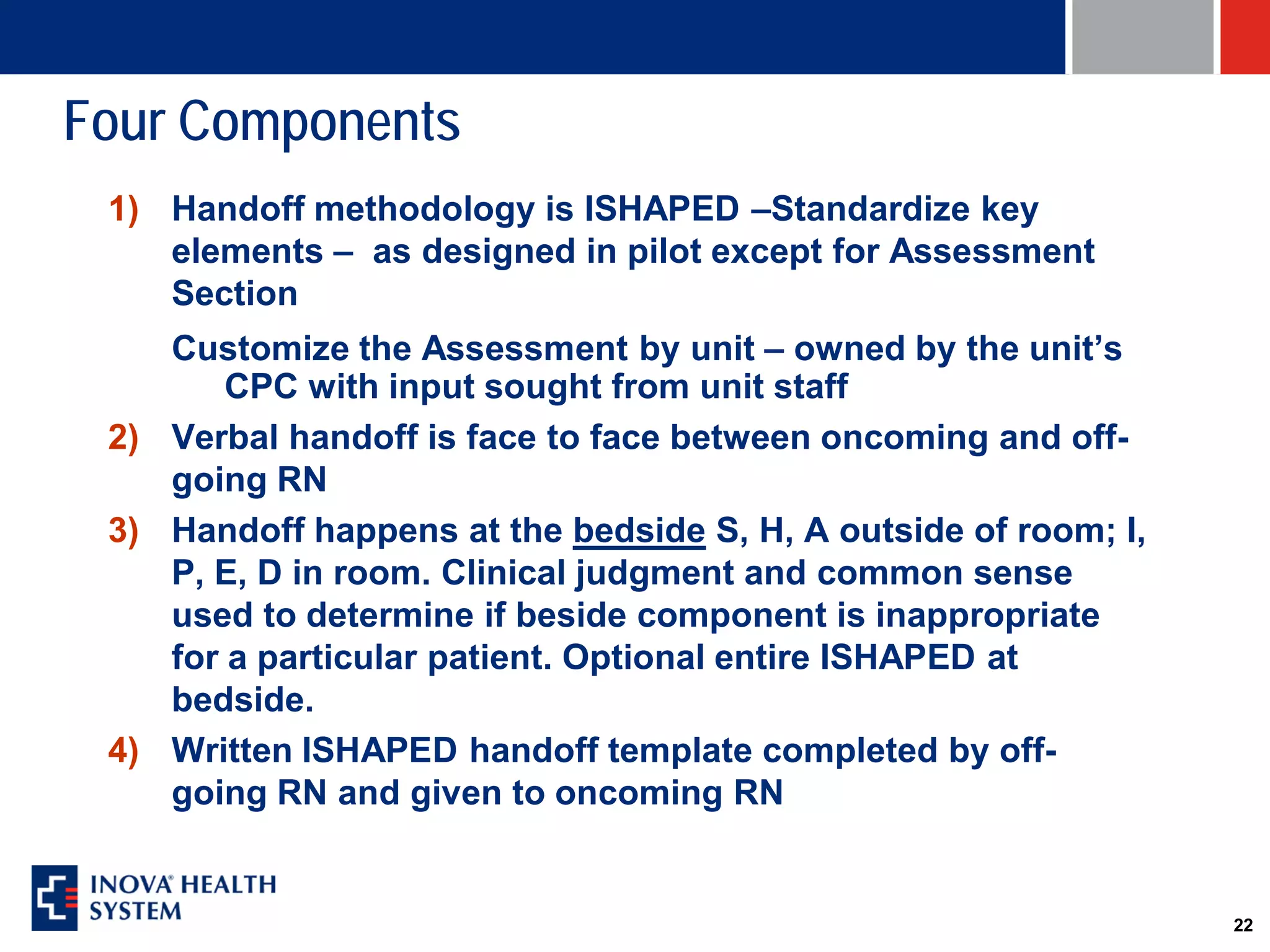
3) Inova's work to standardize handoff processes across its system through a kaizen event, surveys identifying opportunities, and developing education programs with Picker's support.