Downloaded 68 times



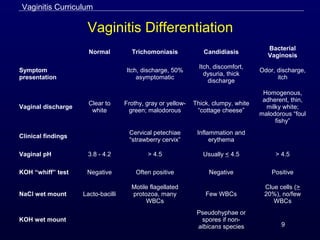


1. Vaginitis is usually characterized by vaginal discharge, vulvar itching, irritation, and odor. Common causes include trichomoniasis, bacterial vaginosis, and vulvovaginal candidiasis. 2. Trichomoniasis is caused by the protozoan Trichomonas vaginalis and is transmitted sexually. Symptoms in women include frothy gray or yellow-green discharge and pruritus. Diagnosis is made by visualizing motile trichomonads on a saline wet mount. 3. CDC-recommended treatment for trichomoniasis is metronidazole 2g orally in a single dose. It is important to treat























































































