3
C
O
N
T
E
N
T
S
• INTRODUCTION
• DEFINITION
•HISTORY
• INDICATIONS
• CONTRAINDICATIONS
• ADVANTAGES
• DISADVANTAGES
• CLASSIFICATION
• COMPOSITION
• METHOD OF
POLYMERIZATION
• TYPES OF COMPOSITE
• CURING OF COMPOSITES
• PROPERTIES
• INDIRECT COMPOSITES
• RECENT ADVANCES IN COMPOSITE
• CLINICAL TECHNIQUES
• FINISHING AND POLISHING
• TUNNEL RESTORATION
• SANDWHICH TECHNIQUE
• CONCLUSION
• REFERENCES
S
E
M
I
N
A
R-
II
4.
4
INTRODUCTION
As esthetic awarenessgrows and becomes more important throughout our society, patients demand highly
esthetic restorations. Esthetic restorative materials must blend into the natural dentition by stimulating the
natural tooth in color, translucence, form, and texture yet also have adequate strength and wear characteristics,
good marginal adaptation and sealing, insolubility, and biocompatibility.
These materials must also remain color stable and maintain external tooth morphology to provide a functional,
lasting esthetic restoration.
They best fulfill the requirements of tooth preservation, excellent esthetics, and durability.
Summitt JB, Robbins JW, Hilton TJ, Schwartz RS, Santos JD. Summitt’s Fundamentals of Operative Dentistry: A Contemporary Approach. 4th ed. Hanover Park, IL:
Quintessence Publishing; 2013.
5.
5
DEFINITION
PHILLIPS’ (SKINNER’S)
Acompound of two or more distinctly different materials with properties that are superior or
intermediate to those of the individual constituents
•STURDEVANT
In materials and science, word composite refers to a solid formed from two or more distinct
phases that have been combined to produce properties superior to or intermediate to those of
individual constituents.
2. Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
1. Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
6.
6
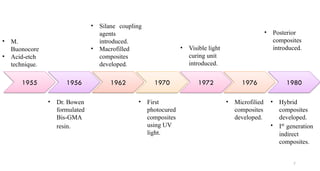
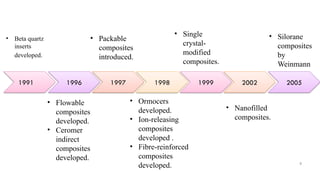
•During the firsthalf of the twentieth century, silicates were the tooth-colored material of choice for
cavity restoration. In 1956, Bowen developed a new type of composite material.
• Bowen’s main innovations were bisphenol-A glycidyl dimethacrylate (bisGMA), a monomer that
forms a cross-linked matrix that is highly durable, and a surface treatment utilizing an organic silane
compound called a coupling agent to bond the filler particles to the resin matrix.
•Current tooth– colored restorative materials continue to use this technology, but many further
innovations have been introduced since 1962.
HISTORY
Shen C, Rawls HR, Esquivel-Upshaw JF. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
INDICATIONS
1. Class I,II, III, IV, V and VI restorations
2. Foundations or core buildups
3. Sealants and preventive resin restorations (conservative composite restorations)
4. Esthetic enhancement procedures: Partial veneers, Full veneers, Diastema closures
5. Temporary or provisional restorations
6. Periodontal splinting
7. Luting of indirect esthetic restorations
8. Interim restorations.
Roberson TM, Heymann HO, Swift EJ. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis, MO: Elsevier; 2018.
12
11.
CONTRAINDICATIONS
1. Access andisolation difficulties.
2. Heavy, abnormal occlusal stresses.
3. Subgingival extensions.
4. Limited operator skill and knowledge.
5. High caries incidence and poor oral hygiene.
Roberson TM, Heymann HO, Swift EJ. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis, MO: Elsevier; 2018.
13
12.
ADVANTAGES
1. Esthetics
2. Conservetooth structure
3. Low thermal conductivity
4. Universal application
5. Adhesion
6. Command set
7. Can be polished at the same appointment
8. Repairable
Roberson TM, Heymann HO, Swift EJ. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis, MO: Elsevier; 2018.
14
16
CLASSIFICATION
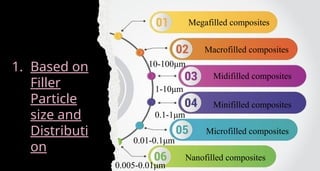
• Based onfiller particle size and distribution (O'BRIEN in 2002)
• Classification of resin based composites and indications for use
• Based on method of polymerization
• Based on the mode of presentation
• Based on use
• Based on their consistency
• Generations of composite resins
15.
Megafilled composites
Macrofilled composites
Midifilledcomposites
Minifilled composites
Microfilled composites
Nanofilled composites
1. Based on
Filler
Particle
size and
Distributi
on
10-100μm
1-10μm
0.1-1μm
0.01-0.1μm
0.005-0.01μm
16.
Shen C, RawlsHR, Esquivel-Upshaw JF. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
19
22
23
Based on themode of presentation
1. Two paste system
2. Single paste system
3. Powder-liquid system
Based on use
1. Anterior composites
2. Posterior composites
3. Core buildup composites
4. Luting composites
21.
24
Based on theirconsistency
1. Light body composite – Flowable composites
2. Medium body composites – Medium viscosity composites like microfilled, hybrid,
microhybrid composites.
3. Heavy body composites – Packable composites
22.
25
4. GENERATIONS OFCOMPOSITE RESINS
• FIRST GENERATION COMPOSITES-
Macroceramic reinforcing phases in an appropriate resin matrix, they have the highest surface
roughness.
• SECOND GENERATION COMPOSITES-
With colloidal and micro ceramic phases in continuous phase, they exhibit best surface texture and
wear resistance better than first generation.
• THIRD GENERATION COMPOSITES-
Hybrid composite in which there is combination of macro and micro ceramics as reinforcers, existing
in 75:25 ratio.
23.
26
• FOURTH GENERATIONCOMPOSITES-
Heat cured, irregularly shaped, highly reinforced composite macro particles with a reinforcing phase
of micro ceramics.
• FIFTH GENERATION COMPOSITES-
Hybrid system in which the continuous resin phase is reinforced with micro ceramics and macro
spherical, highly reinforced, heat cured composite particles.
Surface texture and wear of these materials would be comparable to that of second generation and
physical and mechanical properties comparable to that of fourth generation.
• SIXTH GENERATION COMPOSITES-
Hybrid types in which there is the continuous phase is reinforced with a combination of micro colloidal
ceramics and agglomerates of sintered microceramics.
It exhibits least shrinkage.
24.
(ANSVADA No. 27)describes two types and three classes of composites, as shown by the
following:
Type 1: Polymer-based materials suitable for restorations involving occlusal surfaces
Type 2: Other polymer-based materials
Class 1: Self-cured materials
Class 2: Light-cured materials
Group 1 : Energy applied intra-orally
Group 2: Energy applied extra-orally
Class 3: Dual-cured materials
Sakaguchi RL, Ferracane J, Powers JM, editors. Craig's Restorative Dental Materials. 14th ed. St. Louis: Mosby; 2018
25.
28
COMPOSITION OF COMPOSITES
Thecomponents of composites are:
a. Resin matrix
b. Fillers
c. Coupling agents
d. Coloring agents
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
26.
29
The initialresin matrix was Bisphenol Glycidyl methacrylate (BisGMA) and urethane
dimethacrylate (UDMA).
The BiSGMA/UDMA was viscous and blending of filler particles was difficult, so other
matrix were tried having lower viscosity, such as:
TEGDMA (Triethylene glycol dimethacrylate) The mixture of two of these three resins
provides appropriate viscosity needed for binding of filler particles. BisGMA and
TEGDMA in the ratio of 3:1 is preferred as increase in TEGDMA substantially increases
the polymerization shrinkage.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
Resin Matrix
27.
30
Inorganic Fillers
Thesize of the filler particles vary from composite to composite depending upon the requirements
and needs.
To ensure acceptable esthetics of composites, the translucency of the filler must be similar to tooth
structure. Mostly glasses have refractive index 1.5 which is comparable to dentin 1.52 and enamel
1.62.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
28.
31
ii. Silica: Silicahas been used as filler in many forms as pure silica, fused silica and colloidal silica.
These silica fillers apart from reinforcing the composite, also help in light scattering and light
transmission. Other fillers such as Tricalcium phosphate and Zirconium dioxide have also been
used.
The routinely used fillers are:
i. Quartz: Quartz is extremely hard and to grind it in finer particles is difficult. These were used
in early composites, which were difficult to polish and even abraded the opposing tooth structure.
29.
Fillers provide:
• Strength
•Rigidity
• Hardness
• Increase in modulus of elasticity
• Decrease in coefficient of
thermal expansion
• Decrease in contraction
32
30.
33
Recent composites containcombination of Macro (Barium glass, particle size
0.7–2.0 μm) and micro (Pyrogenic silica, particle size 0.04–0.07 μm) fillers.
These types of fillers provide:
• Better polishing
• Kindness to antagonist tooth
• Good esthetic and chameleon effect
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
31.
34
Silane Coupling Agents
SikriVK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
Provides interfacial bonding between organic matrix and the inorganic filler particle
phases
Precoated the silica filler particles with mononuclear films of silane coupling
agents.
Di-functional
32.
35
ü One endis capable of bonding to hydroxyl groups, which exist along the surface
of silica particles, and other end is capable of co-polymerizing with double bonds
of monomers in the matrix phase.
ü Organic silanes such as γ-methacryloxy propyl trimethoxy silane are commonly
used as coupling agents.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
33.
36
Photoinitiator
Composites arepolymerized with the help of light.
Camphorquinone as photoinitator.
Absorbs photons of light at 470nm.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
34.
38
MACROFILL COMPOSITES
Thefirst type of composites introduced in the early 1960s.
No longer used in clinical practice.
Average particle size is approximately 10-20 µm.
Because of the relatively large size and extreme hardness of the filler particles,
macrofill composites typically exhibit a rough surface texture.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
35.
39
This typeof surface texture causes the restoration to be more susceptible to
discoloration from extrinsic staining.
Macrofill composites have a higher amount of initial wear at occlusal contact
areas than do the microfill or hybrid types.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
36.
40
MICROFILL COMPOSITES
Replacethe rough surface characteristic of conventional composites with a smooth, lustrous
surface similar to tooth enamel.
Contain colloidal silica particles whose average diameter is 0.01 to 0.04 µm.
This small particle size results in a smooth, polished surface in the finished restoration that is less
receptive to plaque or extrinsic staining.
Have an inorganic filler content of approximately 35% to 60% by weight as it cannot be heavily
filled.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
37.
41
Less fillerthan do conventional or hybrid composites, some of their physical and mechanical
characteristics are inferior.
Are clinically highly wear resistant. Also, their low modulus of elasticity may allow
microfill composite restorations to flex during tooth flexure, better protecting the bonding
interface.
Their primary indication is for esthetic areas where this luster is required, such as for direct
resin composite veneers.
There are 2 types of Microfilled composites.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
38.
42
1. HETEROGENEOUS MICROFILL
oBlend of precured microfill composite with uncured material.
o Precured particles are generated by grinding cured composites 10-20 µm sized powder.
o Chemically bonded to new material
o Finely finished.
2. HOMOGENEOUS MICROFILL
o Unmodified microfills
Restoring Class V cervical lesions or defects in which cervical flexure is significant
(eg. Bruxism, clenching, stressful conditions)
39.
HYBRID COMPOSITES
1. Hybridcomposites were developed in an effort to combine the favorable physical
and mechanical properties characteristic of macrofill composites with the smooth
surface typical of the microfill composites.
2. Have an inorganic filler content of approximately 75% to 85% by weight.
3. Smaller average particle size (0.4–1 µm) than that of conventional composites.
40.
5. Can beused for anterior and posterior restorations. The high filler content also
improves the hybrid material’s resistance to internal discoloration.
6. Current versions of hybrid composites also contain ultrasmall nanofillers, resulting in
superior characteristics. These newer versions of hybrid composites are called mini-
nanohybrid composites.
4. Relatively high content of inorganic fillers, the physical and mechanical
characteristics are generally superior to those of conventional composites, hence
called mini-micro composites. Classic versions of hybrid materials exhibit a smooth
“patina-like” surface texture in the finished restoration.
41.
45
NANOFILL COMPOSITES
1. Fillerparticles that are extremely small (0.005–0.01 µm).
2. High filler levels can be generated in the restorative material, which results in good
physical properties and improved esthetics.
3. The small primary particle size also makes nanofills highly polishable. Because of these
qualities, nanofill and nanohybrid composites are the most popular composite restorative
materials in use.
4. These composites have almost universal clinical applicability and are the primary
materials referred to as composites.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
42.
46
FLOWABLE COMPOSITES
1. Havelower filler content and consequently inferior physical properties such as
lower wear resistance and lower strength compared with the more heavily filled
composites.
2. The filler content is reduced which results in a decrease in viscosity.
3. They serve as liner to absorb the shrinkage/ contraction of the overlying
composite restoration.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
43.
47
These materials havethe following features:
• The filler content is 20–25% less than that of the traditional hybrid composites.
• Because of the lesser amount of fillers loading, the flow is increased.
• Stickiness to the instrument, which makes it difficult to smoothen the material.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
44.
The flowable compositesare useful as follows:
• As filling materials in low stress areas.
• As pit and fissure sealing and preventive resin
restorations.
• As liners in proximal boxes of class II preparations.
• For repairing porcelain.
• For rebuilding worn contact areas in composite
restorations.
• Tunnel restorations.
• Core build-up.
• Cementing agents for porcelain restorations.
48
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
50
Flowable composites aregenerally contra-indicated for class I, II and IV restorations,
because of the relatively high stresses in these areas.
Because they can flow into small crevice defects along restoration margins, some
dentists refer to flowable resins as “dental caulk.”
The properties and clinical uses of flowable composite materials are similar to
those of the so-called compomers, which are hybrids between resin composites
and glass ionomer materials
47.
51
PACKABLE COMPOSITES
Packable/condensablecomposites are based on the newly
introduced concept, called PRIMM (polymer rigid
inorganic matrix material).
This system consists of a resin and a ceramic component.
The filler/ inorganic phase instead of being incorporated into
composites as ground particles is present as a continuous
network/scaffold of ceramic fibers.
The fibers are composed of alumina and silicon dioxide.
The diameter of the individual ceramic fiber is less than 2.0
μm.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
48.
52
The consistencyof PRIMM based composites is similar to that of a freshly
triturated mass of silver amalgam.
The composite is inserted into the prepared cavity by carrying and ejecting from a
carrier whose nozzle is preferably made from/coated with wear resistant teflon
polymer.
Packable composites present improved properties over conventional ones, like:
• Increased flexural modulus
• Increased resistance to wear
• Non-stickiness
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
49.
53
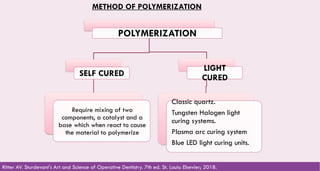
METHOD OF POLYMERIZATION
POLYMERIZATION
SELFCURED
Require mixing of two
components, a catalyst and a
base which when react to cause
the material to polymerize
LIGHT
CURED
Classic quartz.
Tungsten Halogen light
curing systems.
Plasma arc curing system
Blue LED light curing units.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
50.
54
CURING OF COMPOSITES
•After the discontinuation of chemically cured composites, various types of lights
have been used to cure composites.
• A light curing unit with a minimal light output of 550 lux is considered
appropriate for dental use.
51.
55
García et alComposite resins. A review of the materials and clinical indications. Med Oral Patol Oral Cir Bucal 2006;11:E215-20
52.
56
Lehmann A, NijakowskiK et al aimed to determine the
material preferences and analyse the clinical problems
associated with direct compos- ite restorations in a cohort of
dentists.
Authors confirmed that resin-based composites are the most
popular material for direct restoration in many countries.
Although working with this material is difficult and involves
multiple steps, maintaining a dry cavity during bonding, and
material application may affect the therapeutic success and
durability of these restorations. Clinicians need to be attentive
to this issue and be prepared to adapt their decision-making
and consider opting for alternative restorative materials, if
appropriate.
Lehmann A, Nijakowski K et al. Clinical Difficulties Related to Direct Composite Restorations: A Multinational Survey. Int J Dent. 2025; 75(1): 797-806.
58
DEGREE OF CONVERSION(DC)
1. The DC is a measure of the percentage of carbon-carbon double bonds that have
been converted to single bonds to form a polymeric resin.
2. The higher the DC, the better the strength, wear resistance, and many other
properties essential to resin performance.
Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
55.
59
DEGREE OF CONVERSION(DC)
1. The DC is a measure of the percentage of carbon-carbon double bonds that have
been converted to single bonds to form a polymeric resin.
2. The higher the DC, the better the strength, wear resistance, and many other
properties essential to resin performance.
Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
56.
60
1. The LCTEis the rate of dimensional change of a material per unit change in
temperature.
2. The closer the LCTE of the material is to the LCTE of enamel, the lower the chance
for creating voids or openings at the junction of the material and the tooth when
temperature changes occur.
3. The LCTE of modern composites is approximately three times that of tooth
structure.
LINEAR COEFFICIENT OF THERMAL EXPANSION
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
57.
61
WATER SORPTION
1. Watersorption is the amount of water that a material absorbs over time per unit of
surface area or volume.
2. All of the available tooth-colored materials exhibit some water absorption.
3. Materials with higher filler contents exhibit lower water absorption values than
materials with lower filler content.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
58.
62
WEAR RESISTANCE
1. Wearresistance refers to a material’s ability to resist surface loss as a result of
abrasive contact with opposing tooth structure, restorative material.
2. The filler particle size, shape, and content affect the potential wear of composites
and other tooth-colored restorative materials.
3. The location of the restoration in the dental arch and occlusal contact relationships
also affect the potential wear of these materials.
4. Wear resistance of contemporary composite materials is generally good but not as
resistant as amalgam but the difference is getting smaller.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
59.
63
SURFACE TEXTURE
1. Surfacetexture is the smoothness of the surface of the restorative material.
2. The size and composition of the filler particles primarily determine the smoothness
of a restoration, as does the material’s ability to be finished and polished.
3. Although microfill composites historically have offered the smoothest restorative
surface, nanohybrid and nanofill composites also provide surface textures that are
polishable, esthetically satisfying, and compatible with soft tissues.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
60.
64
RADIOPACITY
1. Esthetic restorativematerials must be sufficiently radiopaque so that the
radiolucent image of recurrent caries around or under a restoration can be seen
more easily in a radiograph.
2. Most composites contain radiopaque fillers such as barium glass to make the
material radiopaque.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
61.
65
MODULUS OF ELASTICITY
1.Modulus of elasticity is the stiffness of a material.
2. A material having a higher modulus is more rigid; conversely, a material with a
lower modulus is more flexible.
3. A microfill composite material with greater flexibility may perform better in
certain Class V restorations than a more rigid hybrid composite.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
62.
66
4. This isparticularly true for Class V restorations in teeth experiencing heavy
occlusal forces, where stress concentrations exist in the cervical area. Such stress
can cause tooth flexure that can disrupt the bonding interface. Using a more
flexible material such as a microfill composite allows the restorations to bend
with the tooth, better protecting the bonding interface.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018
63.
67
SOLUBILITY
1. Solubility isthe loss in weight per unit surface area or volume secondary to
dissolution or disintegration of a material in oral fluids, over time, at a given
temperature.
2. Composite materials do not show any clinically relevant solubility.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 6th ed. St. Louis: Elsevier; 2018.
64.
68
Resin composites haveseveral undesirable characteristics that must be overcome to
achieve long-term clinical success. Volumetric shrinkage during polymerization is typically
between 1.5% and 5.0%, which, when the material is placed into a bonded cavity
preparation, generates internal stresses in the composite that create additional stresses
at the bonded tooth-composite interface, potentially leading to marginal defects.
Shrinkage stresses that occur in the early phase of polymerization when the composite
is still relatively fluid are effectively relieved by deformation and flow of the material.
However, stresses occurring later in the process, after the material has acquired
significant rigidity (called gelation), are not relieved by material flow. These residual
stresses may leave the composite weakened and may reduce the adhesion to the tooth.
Summitt’s Fundamentals of Operative Dentistry A Contemporary Approach - 4th Edition
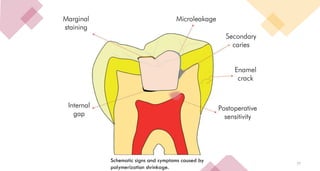
POLYMERIZATION SHRINKAGE
65.
69
These stresses alsomay cause gap formation at the cavosurface margins, especially
at those with the weakest bonds (usually dentin or cementum). Marginal gaps may
result in microleakage, sensitivity, staining at the margins of the restoration, and
recurrent caries.
There are five primary strategies that can be used to reduce polymerization
shrinkage stress:
The first is to create a relatively thick primed layer with the chosen dentin bonding
agent.
The second strategy is to use a thin liner (0.5 mm) of resin modiied glass ionomer
under the composite resin restoration.
Summitt’s Fundamentals of Operative Dentistry A Contemporary Approach - 4th Edition
66.
70
The third optionis to place a thin layer (0.5 mm) of Flowable composite resin as a
liner.
A fourth concept that may be used to reduce shrinkage stress is the use of “soft-start”
polymerization. To prolong the gel phase of the setting reaction of the composite resin
material. The theory is that the longer the setting composite can maintain a gel or
Flowable condition, the better it can distribute the stresses resulting from shrinking .By
the use of ramped lights, pulse curing, or simply holding the curing light some
distance from the material for the initial exposure.
The Final approach to reduce stress is to place the composite resin in increments.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
67.
71
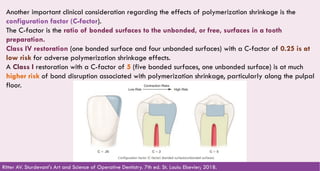
Another important clinicalconsideration regarding the effects of polymerization shrinkage is the
configuration factor (C-factor).
The C-factor is the ratio of bonded surfaces to the unbonded, or free, surfaces in a tooth
preparation.
Class IV restoration (one bonded surface and four unbonded surfaces) with a C-factor of 0.25 is at
low risk for adverse polymerization shrinkage effects.
A Class I restoration with a C-factor of 5 (five bonded surfaces, one unbonded surface) is at much
higher risk of bond disruption associated with polymerization shrinkage, particularly along the pulpal
floor.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
68.
72
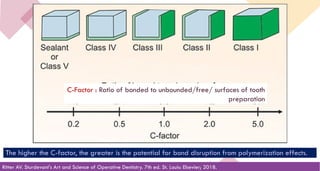
C-Factor : Ratioof bonded to unbounded/free/ surfaces of tooth
preparation
The higher the C-factor, the greater is the potential for bond disruption from polymerization effects.
Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
78
Guidelines to minimizechances of composite failure:
• Tooth preparation should be kept as small as possible since composite in bulk leads to failure.
• Avoid sharp internal line angles in tooth preparation.
• Deeper preparations should be given base of calcium hydroxide or glass ionomer cement.
• Strict isolation regime is to be followed.
• Avoid inadequate curing, because it leads to hydrolytic breakdown of composites.
• Use small increments, holding each increment with teflon coated instruments.
• Fill proximal box separately and create proper contact areas.
• Composite, especially at beveled areas, should be finished and polished properly
75.
REFERENCES
1. Sikri VK.Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
2. Shen C, Rawls HR, Esquivel-Upshaw JF, editors. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
3. Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
4. Sakaguchi RL, Ferracane J, Powers JM, editors. Craig's Restorative Dental Materials. 14th ed. St. Louis: Mosby; 2018.
5. Lehmann A, Nijakowski K et al. Clinical Difficulties Related to Direct Composite Restorations: A Multinational Survey. Int J Dent.
2025; 75(1): 797-806.
6. Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
7. Chandrashekar V, Rudrapati L et al. Incremental techniques in direct composite restoration. J Conserv Dent. 2017; 20(6): 386–391.
77.
81
INDIRECT COMPOSITES
Agathian R,Manoharan PS et al. Indirect Resin Composite - A Literature Review. J Adv Clin Res. 2021; 8(1): 13-18.
78.
82
IRCs are restorationsthat are fabricated outside the oral cavity. Most of the IRCs are
made on the removable dies of the prepared tooth inside the laboratory. IRCs replace
various restorations. IRC gives an esthetic substitute to ceramic materials for the posterior
tooth.
79.
83
CHARACTERISTIC FEATURES OFIRC
POLYMERIZATION SHRINKAGE: Methacrylate is the material which causes
polymerization shrinkage. It results in gap formation and micro leakage of the
restorations. The use of direct composite in the larger posterior restorations remains a
challenge because of the polymerization shrinkage.
Logurecio et al in 2004 and Thonemann et al in 1999 observed that direct composites
could not resist the stresses due to polymerization in margins of enamel free cavities .
Studies have shown that polymerization shrinkage is less in indirect composites when
compared to the direct composite restorations. It is due to the curing mechanisms. It
includes light, heat, pressure which takes place outside the oral cavity.
80.
84
CONTACTS AND CONTOURS:Establishing a correct proximal contour and ensuring a
firm contact with the adjacent tooth in direct restorations is a challenge. Indirect
composite restorations provide excellent proximal contacts and contour since the
fabrication is done outside the oral cavity, which makes it superior from the direct
composites.
81.
85
WEAR: Direct compositerestorations exhibit excessive wear in areas of high occlusal
stress. The major cause of clinical failure of the direct restoration was due to poor
wear resistance.
This can be overcome by curing the composite resin extra-orally with the help of
secondary/additional curing using light, pressure, vacuum, heat, inert gas, or a
combination of these methods resulting in a dense well-cured restoration.
Such restorations can be finished and polished better and can then be cemented to the
prepared cavity resulting in a dense well-cured restoration. The physical properties of
such restorations are greatly improved.
82.
86
DISADVANTAGES OF IRCRESTORATIONS
Expensive
Increased Tooth reduction: Indirect restorations may require more tooth reduction as
compared to direct composites to create a path of insertion and removal. It is mainly
due to the divergent tooth preparation and other tooth preparation reduction
requirements.
Difficult for alteration: It is difficult to modify or add extrinsic color at the chair side.
Luting: The thin layer of luting resin cement is liable for shrinkage at the tooth–
restoration interface. The luting resin cement which is applied during the luting
procedure is responsible for the polymerization shrinkages.
83.
87
Indications of IRC
1.Laminate veneers.
2. Inlays and onlays.
3. Jacket crowns.
4. Implant supported restorations.
5. Full coverage crowns.
6. Patients with bone loss.
7. Patients with poor periodontal support requiring occlusal coverage.
8. Fiber-reinforced bridges or retainers.
Contraindications of IRC
9. Patients with parafunctional habits.
10.Inability to isolate the working area because luting of irc is technique sensitive.
11.Teeth with heavy wear and tear due to tmj and occlusal disharmony
84.
88
Steps of CompositeRestoration
The steps involved in restoration of tooth with composite materials include:
1. Preparation of the operative site
2. Shade selection
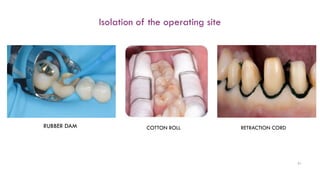
3. Isolation of the operating site
4. Tooth preparation
5. Acid etching
6. Bonding agent application
7. Insertion of composite material
8. Curing
9. Finishing and Polishing
85.
Preparation of theOperative Site
89
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
86.
90
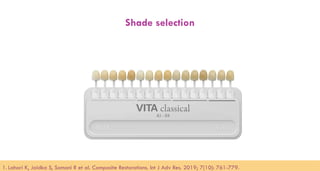
Shade selection
1. LahariK, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
92
Tooth Preparation
Tooth preparationfor a composite restoration includes the following:
• Removing the fault, defect old material or friable tooth structure.
• Creating prepared enamel margins of 90 degree or greater.
• Creating 90 degree cavosurface margins on root surface.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
89.
93
Types of ToothPreparation
The designs of tooth preparations for composites are:
• Conventional
• Beveled conventional
• Modified
• Box only
• Slot preparations
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
90.
94
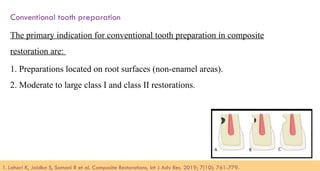
Conventional tooth preparation
Theprimary indication for conventional tooth preparation in composite
restoration are:
1. Preparations located on root surfaces (non-enamel areas).
2. Moderate to large class I and class II restorations.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
91.
95
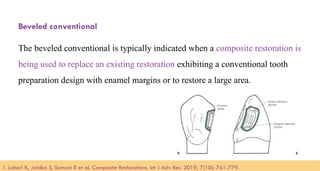
Beveled conventional
The beveledconventional is typically indicated when a composite restoration is
being used to replace an existing restoration exhibiting a conventional tooth
preparation design with enamel margins or to restore a large area.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
92.
96
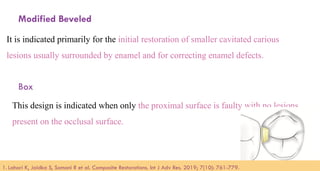
Modified Beveled
It isindicated primarily for the initial restoration of smaller cavitated carious
lesions usually surrounded by enamel and for correcting enamel defects.
Box
This design is indicated when only the proximal surface is faulty with no lesions
present on the occlusal surface.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
93.
97
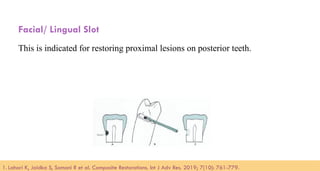
Facial/ Lingual Slot
Thisis indicated for restoring proximal lesions on posterior teeth.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
94.
98
Acid Etching
Etching isdefined as the process of increasing the surface reactivity by demineralizing the superficial calcium
layer and thus creating the enamel tags.
Mechanism of Action:
After tooth preparation, smear layer which constitutes hydroxyapatite, altered collagen with an external surface
formed by denatured collagen is formed on the surface of tooth. When an etchant is applied to the tooth surface, it
dissolves the smear layer and penetrates it. There is preferential dissolution of hydroxyapatite crystals from
enamel and dentin that results in microporous surface topography.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
95.
99
1. Lahari K,Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
96.
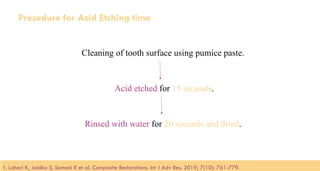
100
Procedure for AcidEtching time
Cleaning of tooth surface using pumice paste.
Acid etched for 15 seconds.
Rinsed with water for 20 seconds and dried.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
97.
101
Bonding Agent Application
•Dentin adhesion relies primarily on the penetration of adhesive monomers into
the filigree of collagen fibres left exposed by acid etching.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
104
Fathpour K, BazazzadeA, Mirmohammadi H
(2021) compared microleakage of cervical
restorations using universal bonding and two-step
self-etch adhesive with or without enamel etching
through a dye penetration testing method.
Authors deduced that selective etching of enamel
will decrease enamel microleakage. G-Premio
Bond shows better microleakage results in
comparison to Clearfil SE Bond in dentinal
margins.
Fathpour K, Bazazzade A, Mirmohammadi H. A Comparative Study of Cervical Composite Restorations Microleakage Using Dental Universal
Bonding and Two-step Self-etch Adhesive. J Contemp Dent Pract 2021;22(9):1035–1040.
101.
105
Insertion of CompositeRestoration
Composite resins can be inserted in the prepared cavities either in a bulk or
incremental pattern depending on the site of restoration.
1. Lahari K, Jaidka S, Somani R et al. Composite Restorations. Int J Adv Res. 2019; 7(10): 761-779.
102.
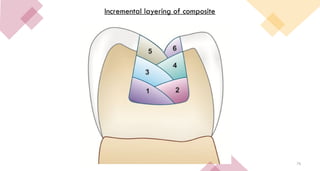
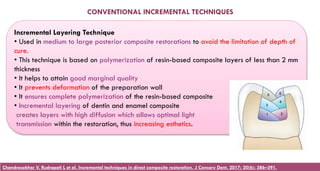
Incremental Layering Technique
•Used in medium to large posterior composite restorations to avoid the limitation of depth of
cure.
• This technique is based on polymerization of resin-based composite layers of less than 2 mm
thickness
• It helps to attain good marginal quality
• It prevents deformation of the preparation wall
• It ensures complete polymerization of the resin-based composite
• Incremental layering of dentin and enamel composite
creates layers with high diffusion which allows optimal light
transmission within the restoration, thus increasing esthetics.
CONVENTIONAL INCREMENTAL TECHNIQUES
Chandrasekhar V, Rudrapati L et al. Incremental techniques in direct composite restoration. J Conserv Dent. 2017; 20(6): 386–391.
103.
107
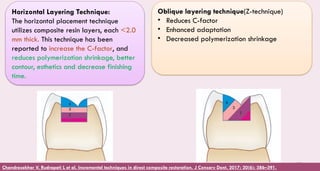
Horizontal Layering Technique:
Thehorizontal placement technique
utilizes composite resin layers, each <2.0
mm thick. This technique has been
reported to increase the C-factor, and
reduces polymerization shrinkage, better
contour, esthetics and decrease finishing
time.
Oblique layering technique(Z-technique)
• Reduces C-factor
• Enhanced adaptation
• Decreased polymerization shrinkage
Chandrasekhar V, Rudrapati L et al. Incremental techniques in direct composite restoration. J Conserv Dent. 2017; 20(6): 386–391.
104.
108
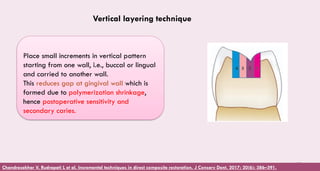
Place small incrementsin vertical pattern
starting from one wall, i.e., buccal or lingual
and carried to another wall.
This reduces gap at gingival wall which is
formed due to polymerization shrinkage,
hence postoperative sensitivity and
secondary caries.
Vertical layering technique
Chandrasekhar V, Rudrapati L et al. Incremental techniques in direct composite restoration. J Conserv Dent. 2017; 20(6): 386–391.
105.
110
Curing
The four maintypes of photopolymerization sources currently available are visible
lights such as
1. Quartz tungsten halogen lamps
2. Plasma arc lamps
3. Argon ion lasers
4. Light emitting diodes.
• Photopolymerization is a technique that uses light (visible or ultraviolet) to initiate and
propagate a polymerization reaction to form a linear or crosslinked polymer structure.
106.
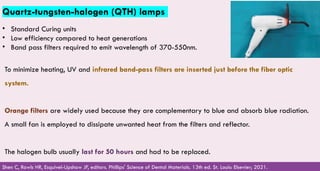
Quartz-tungsten-halogen (QTH) lamps
•Standard Curing units
• Low efficiency compared to heat generations
• Band pass filters required to emit wavelength of 370-550nm.
Shen C, Rawls HR, Esquivel-Upshaw JF, editors. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
To minimize heating, UV and infrared band-pass filters are inserted just before the fiber optic
system.
Orange filters are widely used because they are complementary to blue and absorb blue radiation.
A small fan is employed to dissipate unwanted heat from the filters and reflector.
The halogen bulb usually last for 50 hours and had to be replaced.
107.
112
Sikri VK. Textbookof Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
108.
113
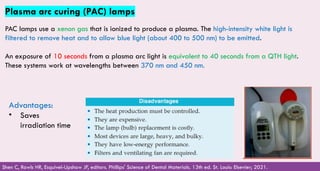
Plasma arc curing(PAC) lamps
PAC lamps use a xenon gas that is ionized to produce a plasma. The high-intensity white light is
filtered to remove heat and to allow blue light (about 400 to 500 nm) to be emitted.
An exposure of 10 seconds from a plasma arc light is equivalent to 40 seconds from a QTH light.
These systems work at wavelengths between 370 nm and 450 nm.
Shen C, Rawls HR, Esquivel-Upshaw JF, editors. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
Advantages:
• Saves
irradiation time
109.
114
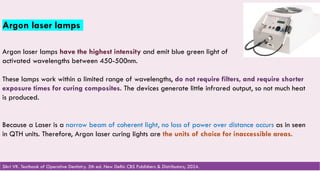
Argon laser lamps
Argonlaser lamps have the highest intensity and emit blue green light of
activated wavelengths between 450-500nm.
These lamps work within a limited range of wavelengths, do not require filters, and require shorter
exposure times for curing composites. The devices generate little infrared output, so not much heat
is produced.
Because a Laser is a narrow beam of coherent light, no loss of power over distance occurs as in seen
in QTH units. Therefore, Argon laser curing lights are the units of choice for inaccessible areas.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
110.
115
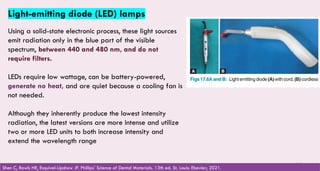
Light-emitting diode (LED)lamps
Using a solid-state electronic process, these light sources
emit radiation only in the blue part of the visible
spectrum, between 440 and 480 nm, and do not
require filters.
LEDs require low wattage, can be battery-powered,
generate no heat, and are quiet because a cooling fan is
not needed.
Although they inherently produce the lowest intensity
radiation, the latest versions are more intense and utilize
two or more LED units to both increase intensity and
extend the wavelength range
Shen C, Rawls HR, Esquivel-Upshaw JF. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
111.
116
THE TECHNIQUES OFCURING COMPOSITES
Soft Start
Low intensity curing is utilized initially followed by a high intensity curing. Various light
curing units automatically provide one or more soft-start exposure sequences.
Soft-start polymerization is divided into three techniques: STEPPED, RAMPED, AND
PULSE-DELAY.
Stepped: The restoration is initially cured at low intensity to contour and shape the
restoration. It is followed by second exposure to completely cure the finished
restoration.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
112.
117
Ramped: In thismethod, intensity is gradually increased or “ramped up.” The intensity is
increased with time either by bringing the light toward the tooth from a distance or using
a curing light designed to increase in intensity with time.
Pulse Delay: In the pulse-delay method, a series of exposure pulses is used, each
separated by a rest period. An initial exposure of up to 1 J/cm2
is considered to be
most efficient in reducing shrinkage stresses. During the rest period, polymerization
reaction occurs at a reduced rate.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
113.
118
High Intensity
High-intensity curingallows for shorter exposure times for a given depth of cure. A depth of 2.0 mm can
be cured in 10 seconds with a Plasma arc light and 5 seconds with an Argon laser-curing light, as
compared with 40 seconds by a Quartz tungsten halogen lamp.
Extra-Oral Curing
Usually, extra-oral curing is used for the fabrication of indirect composite restorations that are
processed in the laboratory. These laboratory photocuring units work with various combinations of light,
heat, pressure, and vacuum to increase the degree of polymerization and wear resistance of
composites.
Sikri VK. Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
114.
119
TECHNIQUE AND LAMPMAINTENANCE
1. A curing lamp with a wavelength range strongly overlapping the absorbance range of the
resin photoinitiation system must be selected.
2. Intensity of light decreases with distance to the log scale; therefore, the lamp tip must be
placed and held at the minimal distance possible throughout the exposure interval (20
seconds or more).
Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
115.
120
3. Curing angleis critical, since maximal intensity is delivered perpendicular (90°) to the
resin surface therefore, the lamp tip must be placed and held as close as possible to 90°
throughout the exposure interval.
4. Lamp intensity should be evaluated frequently and adjustments made to ensure
sufficient radiant energy influx (about 16 J/cm2 ) for adequate curing.
Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
SAFETY PRECAUTIONS FORUSING CURING LAMPS
The light emitted by curing units can cause retinal damage if a person looks
directly at the beam for an extended period or even for short periods in the case
of lasers. To avoid such damage, never look directly into the light tip and
minimize observation of the reflected light for longer periods
Protective eyeglasses and various types of shields that filter the light are
available for increased protection for both clinical personnel and patients.
124
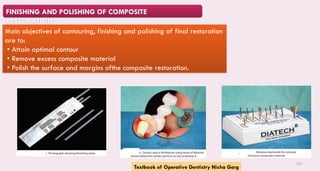
FINISHING AND POLISHINGOF COMPOSITE
RESTORATIONS
Main objectives of contouring, finishing and polishing of final restoration
are to:
• Attain optimal contour
• Remove excess composite material
• Polish the surface and margins ofthe composite restoration.
Textbook of Operative Dentistry Nisha Garg
127
GIOMERS
•Giomer is hybridof words “glass ionomers” and “composite”.
•Giomers have properties of both glass ionomers (Fluoride release, fluoride recharge)
and resin composite (excellent esthetics, easy polishability, biocompatibility).
•Characterized by Pre-Reacted Glass-Ionomer (PRG) technology.
123.
• There isa pre reaction of Fluoroalumino silicate glass fillers with Polyacrylic acid, the
reaction produce a glass ionomer which is more stable.
• This phase is called “WET SILICEOUS HYDROGEL”
• This material is freeze dried, milled, treated with silane and then round to produce
PRG fillers, then these glass fillers are added to the resin matrix (GIOMER)
124.
PROPERTIES
- F releaseand recharge
- Excellent esthetics
- Easy polishability
- Light activated and require use of BONDING
AGENT to adhere to tooth structure
PRG TECHNOLOGY is used in production of two types of
fillers.
• F- PRG : (Fully pre reacted giomers)
e.g., Reactmer (Shofu)
• S-PRG: (Surface pre reacted giomers)
e.g., Beautiful (Shofu)
125.
INDICATIONS
Root caries
Non cariouscervical lesions
Class V cervical lesions
Primary tooth caries
CONTRAINDICATIONS
Class I lesions (decrease wear resistance)
Yap & Mok: Surface Finish of a New Hybrid Aesthetic Restorative Material. Operative Dentistry,
2002, 27, 161-166
126.
COMPOMER
• Polyacid modifiedcomposite resin
• Provide the combined benefits of composites (the “comp” in their name) and glass ionomers
(“omer”)
• Fluoride release of GIC and durability of composite
• Composition- ion leach able glass, sodium fluoride, polyacid modified monomer
but no water.
• Setting reaction- free radical polymerization reaction
• Do not have the ability to bond to hard tooth tissues
• The delayed (post-cure and post-water-sorption) acid-base reaction is speculative
and probably insignificant.
N. Dorin Ruse. What Is a “Compomer”? J Can Dent Assoc 1999; 65:500-4
127.
• Based ontheir structure and properties, these materials belong to the class of dental composites.
• Often erroneously referred to as “hybrid glass ionomers”, “light-cured GICs” or “resin-modified glass
ionomers”along with the “genuine” resin-modified GICs.
• The proposed nomenclature for these materials as polyacid-modified composite resins.
N. Dorin Ruse. What Is a “Compomer”? J Can Dent Assoc 1999; 65:500-4
128.
133
Clinical Usage Theyare preferred in anterior proximal and cervical restorations (Class III or V)
cavities as an alternative to composite and glass ionomer cements.
Disadvantages
• Require use of bonding agent
• Technique sensitive
• Limited fluoride release
• Microleakage more than resin modified
glass ionomers
• Expansion of matrix due to water sorption
• Physical properties decrease with time.
Advantages
• Optimal esthetics
• Easy to handle Easy to polishing
• Easy to place
• Require no mixing
• Bond strength is higher than glass ionomers.
Textbook of Operative Dentistry Nisha garg
129.
134
ORGANICALLY MODIFIED CERAMIC(ORMOCER)
ORMOCER is an organically modified nonmetallic inorganic composite material.
• They are high molecular weight, relatively low viscosity crosslinking molecules and flexible.
• The inorganic network provides abrasion resistance through its glass-like structure and low water.
• Sorption due to its hydrophobicity and low-level polymerization shrinkage is due to large spacing
between crosslinks.
1.Garg N, Garg A. Textbook of Operative Dentistry. 4th ed. New Delhi: Jaypee Brothers Medical Publishers; 2020.
2.Sharma Y. Recent advances in composite resins- an overview. Asian J Biomed Pharmaceut Sci. 2023;13(99):175-179.
130.
135
Indications
1. As aliner of class I and II cavities.
2. Restoration of GV BLACKS class I, II, V cavities.
3. Reconstruction of traumatically damaged anteriors
4. Splinting of loose teeth
5. As a extended fissure sealant
6. Fabrication of composite inlay
7. Core build up
Contraindications
In areas where esthetics is of prime importance.
Sharma Y. Recent advances in composite resins- an overview. Asian J Biomed Pharmaceut Sci. 2023;13(99):175-179.
131.
136
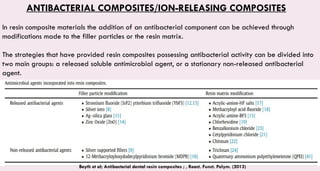
ANTIBACTERIAL COMPOSITES/ION-RELEASING COMPOSITES
Inresin composite materials the addition of an antibacterial component can be achieved through
modifications made to the filler particles or the resin matrix.
The strategies that have provided resin composites possessing antibacterial activity can be divided into
two main groups: a released soluble antimicrobial agent, or a stationary non-released antibacterial
agent.
Beyth et al; Antibacterial dental resin composites ; , React. Funct. Polym. (2013)
132.
137
CHLORHEXIDINE
Though chlorhexidine hasshown
antibacterial properties but its
addition to composites has been
unsuccessful because of the following
reasons:
• Weakening of the physical
properties of composites.
• Release chemicals which show toxic
affects.
• Temporary antibacterial activity.
METHACRYLOYLOXYDECYL PYRIDINIUM
BROMIDE (MDPB)
Use of methacryloyloxydecyl pyridinium bromide
(MDPB) was recommended by Imazato in 1994.
It has the following features:
•Its antibacterial property remains constant and
permanent.
• It has shown to be effective against
streptococci.
• It does not have adverse effect on the physical
properties of Bis-GMA based composites.
• On polymerization, it forms chemical bond to
the resin matrix, therefore, no release of any
antibacterial component takes place.
Silver
Silver ions cause structural damage to the
bacteria. In these composites, the antibacterial
property is due to direct contact with bacteria
and not because of release of silver ions.
Textbook of Operative Dentistry Nisha garg
133.
138
SMART COMPOSITE
•It isa light activated alkaline, nano-filled glass restorative material, which releases calcium, fluoride
and hydroxyl ions when intraoral pH values drop below the critical pH of 5.5 and counteract the
demineralization of the tooth surface and help in remineralization.
•The material can be adequately cured in bulk thickness up to 4mm. It is recommended for the
restoration of class I and class II lesions in both primary and permanent teeth.
•Smart composites containing ACP (amorphous calcium phosphate)
•ACP when integrated into in a composite material, will have an extended time release nature to act
as a source for calcium and phosphate which will be useful for preventing caries
Vertika GuptaSmart materials in dentistry: A reviewInternational Journal of Advance Research and Development (Volume3, Issue6)
134.
139
EXPANDING MATRIX RESINSFOR COMPOSITES
•Composites show polymerization shrinkage on curing which can result in marginal leakage,
postoperative sensitivity and secondary caries. Therefore, slight expansion of the composite during
polymerization is desired to reduce these effects.
•For this, Spiro orthocarbonates (SOCs) are added in composites because they expand on
polymerization. Epoxy resins contract 3.4 percent and SOCs expand 3.6 percent. Both are mixed to
achieve desired expansion
Textbook of Operative Dentistry Nisha garg
135.
140
FIBRE-REINFORCED COMPOSITE
Fiber-reinforced composites(FRCs) are composite materials with three diferent components: the matrix
(continuous phase), the fibers (dispersed phase), and the zone in between (interphase).
FRC materials present high stifness and strength per weight when compared with other structural
materials along with adequate toughness.
Fibre reinforced composite can be classified according to the type of fibre incorporation (glass, carbon
or polyethylene),
the fibre architecture (Mesh, Unidirectional, Weave, Braid, Leno Weave) and
depending on the method of incorporation of fibre.
Aniket Kumar et al. A Review on Fibre Reinforced Composite Resins; Annals of Prosthodontics and Restorative Dentistry, January-March,2016;2(1):
11-16
136.
141
They offer manyadvantages:
• Non-corrosiveness
• Translucency
• Good bonding properties
• Repair facility
• Facility for both office and laboratory
preparation
Applications in dentistry:
• periodontal splinting
• orthodontic retention
• Fiber reinforced post crowns
• Reinforcement and repair of removable
partial denture
• Repair of fixed partial denture
Textbook of Operative Dentistry - Vimal Sikri - 4th Edition (2016)
137.
142
NANOCOMPOSITE
•When inorganic phasesin an organic/inorganic composite become nanosized (range 0.1–100 nm),
they are called nanocomposites.
•Nanofillers are capable of increasing the overall filler level due to their small particlesizes.
•Increase in filler level results in significant reduction of polymerization shrinkage and dramatically
improve the physical properties of nanocomposites.
•Filtek supreme contains nanometric particles (nanomers) and nanoclusters(ncs).
•Premise is a nanohybrid composed of 3 different types of filler components: nonagglomerated
“discrete” silica nanoparticles, prepolymerized fillers (ppf), and barium glass fillers.
•Ceram-x is an ormocer-based, nanoceramiccomposite. Ceram-x contains glass fillers (1.1–1.5 μm) and
methacrylate modified silicon-dioxide-containing nanofiller (10 nm).
Textbook of Operative Dentistry - Vimal Sikri - 4th Edition (2016)
138.
154
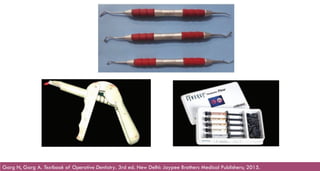
INSERTION OF THECOMPOSITE
Instruments Used for Composite Insertion
Hand instruments: Hand instruments used for placing composites are usually made up of coating with
Teflon so as to avoid sticking of composite to the instrument.
Composite gun: Composite gun is made up of plastic. It is commonly used with composite filled
ampules. For use composite ampules are fitted in the gun and the pressure is applied so that composite
comes out from the ampule.
Syringe: Composite syringe usually carries the low viscosity composite which can easily flow through
needle. This technique has advantage of providing an easy way for placement of composite with
decreased chances of air trapping.
Garg N, Garg A. Textbook of Operative Dentistry. 3rd ed. New Delhi: Jaypee Brothers Medical Publishers; 2015.
139.
155
Garg N, GargA. Textbook of Operative Dentistry. 3rd ed. New Delhi: Jaypee Brothers Medical Publishers; 2015.
140.
156
Irrespective of locationof restoration, composites should be placed and polymerized in increments. This
ensures complete polymerization of the whole composite mass and aids in the anatomical build-up of
the restoration.
Each increment should not be more than 2 mm in thickness, because it is difficult to cure and results in
more polymerization shrinkage stress.
Textbook of Operative Dentistry Nisha Garg
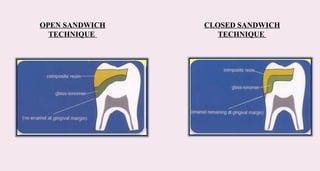
SANDWICH TECHNIQUE
• Developedby McLean
• Also called the LAMINATE or BILARED TECHNIQUE.
• Refers to a laminated restoration using GIC to replace dentin and composite to replace
enamel.
• Combines the most favorable attributes of two restorative materials i.e. translucency,
aesthetics, durability and higher flexural strength of composite resin with good adhesiveness
and anti-cariogenic properties of GIC.
Raghu R. Conservative Dentistry. New Delhi: CBS Publishers & Distributors; 2017.
161
CONCLUSION
Composites have accquireda prominent place among the filling materials employed in
direct techniques. Their considerable aesthetic possibilities give to rise to various
therapeutic indications.
Nonetheless it should not be forgotten that they are highly technique sensitive hence
isolation, its correct indication, choice of right composite for each situation , use of proper
bonding procedure and curing are essential for the satisfactory clinical results.
145.
REFERENCES
1. Sikri VK.Textbook of Operative Dentistry. 5th ed. New Delhi: CBS Publishers & Distributors; 2024.
2. Shen C, Rawls HR, Esquivel-Upshaw JF, editors. Phillips' Science of Dental Materials. 13th ed. St. Louis: Elsevier; 2021.
3. Ritter AV. Sturdevant's Art and Science of Operative Dentistry. 7th ed. St. Louis: Elsevier; 2018.
4. Sakaguchi RL, Ferracane J, Powers JM, editors. Craig's Restorative Dental Materials. 14th ed. St. Louis: Mosby; 2018.
5. Lehmann A, Nijakowski K et al. Clinical Difficulties Related to Direct Composite Restorations: A Multinational Survey. Int J Dent. 2025;
75(1): 797-806.
6. Phillips RW. Skinner's Science of Dental Materials. 9th ed. Philadelphia: Saunders; 1991.
7. Sharma Y. Recent advances in composite resins- an overview. Asian J Biomed Pharmaceut Sci. 2023;13(99):175-179.
8. Chandrashekar V, Rudrapati L et al. Incremental techniques in direct composite restoration. J Conserv Dent. 2017; 20(6): 386–391.
9. Garg N, Garg A. Textbook of Operative Dentistry. 3rd ed. New Delhi: Jaypee Brothers Medical Publishers; 2015.