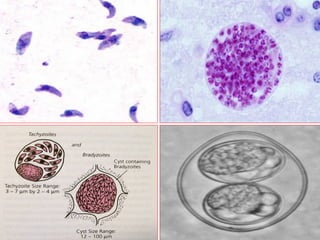
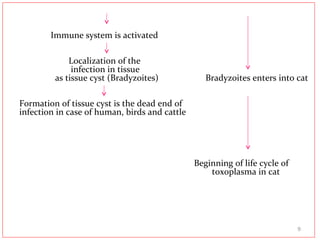
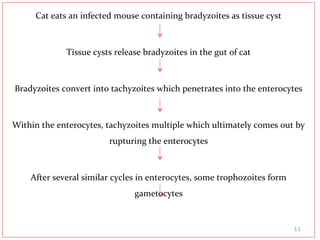
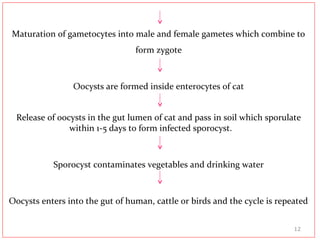
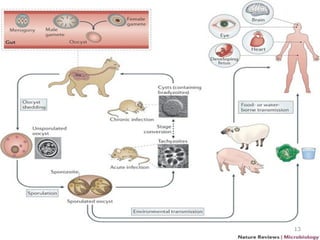
Toxoplasma gondii is an obligate intracellular parasite that infects many mammals worldwide. It has three infectious forms - oocysts, tachyzoites, and bradyzoites. Humans can be infected by ingesting undercooked meat, contaminated food or water, or from a mother to fetus. The parasite forms tissue cysts that the immune system usually keeps dormant. However, it can reactivate and cause severe illness in immunocompromised individuals. While most infections are asymptomatic, congenital infection poses risks like blindness, brain damage, and death for fetuses. Diagnosis involves antibody tests and microscopy. Treatment uses pyrimethamine and sulfadiazine to prevent complications in high-






















![[Micro] mycobacterium tuberculosis](https://cdn.slidesharecdn.com/ss_thumbnails/knwspassdmixhofx5ycy-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)













































