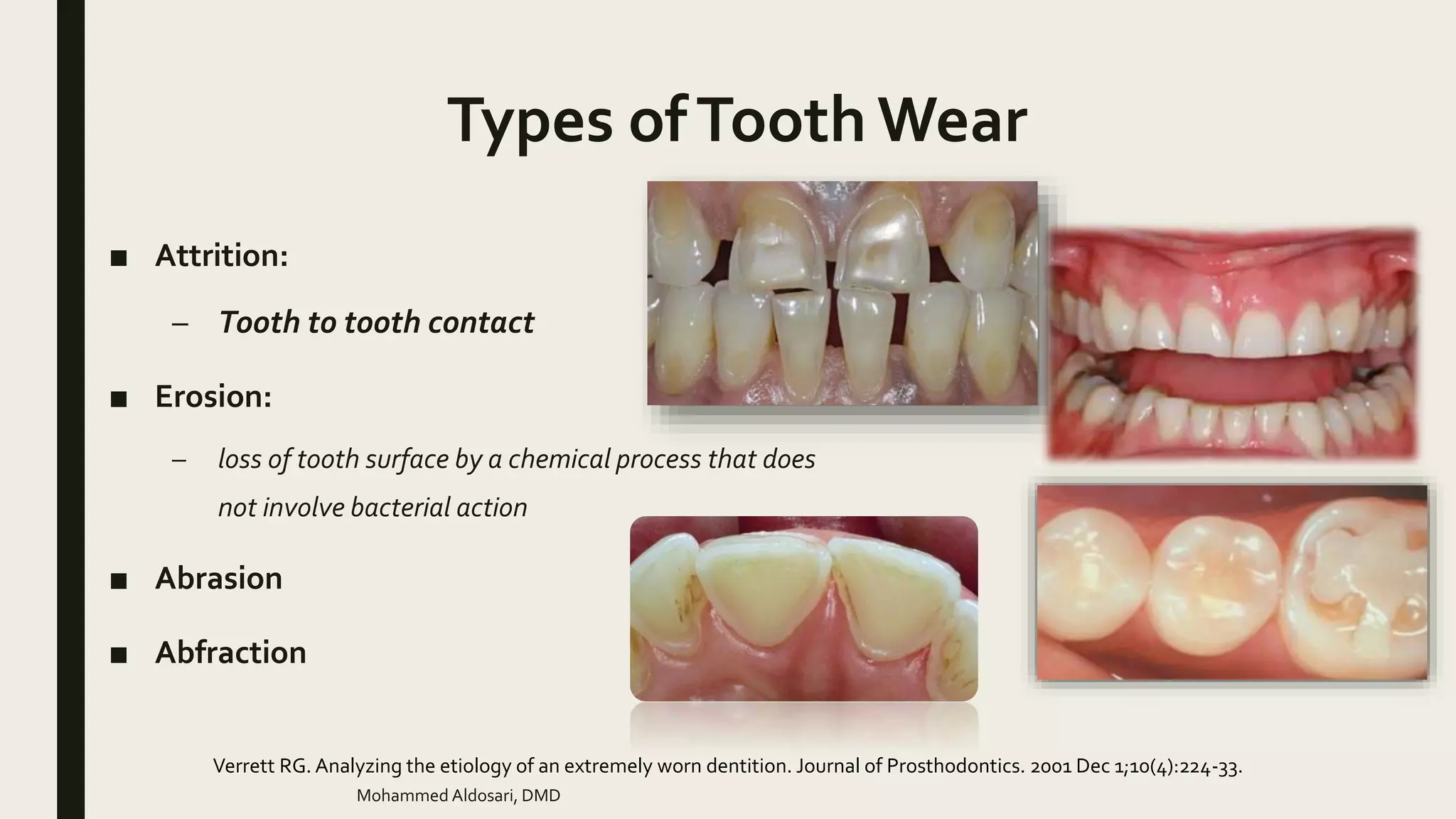
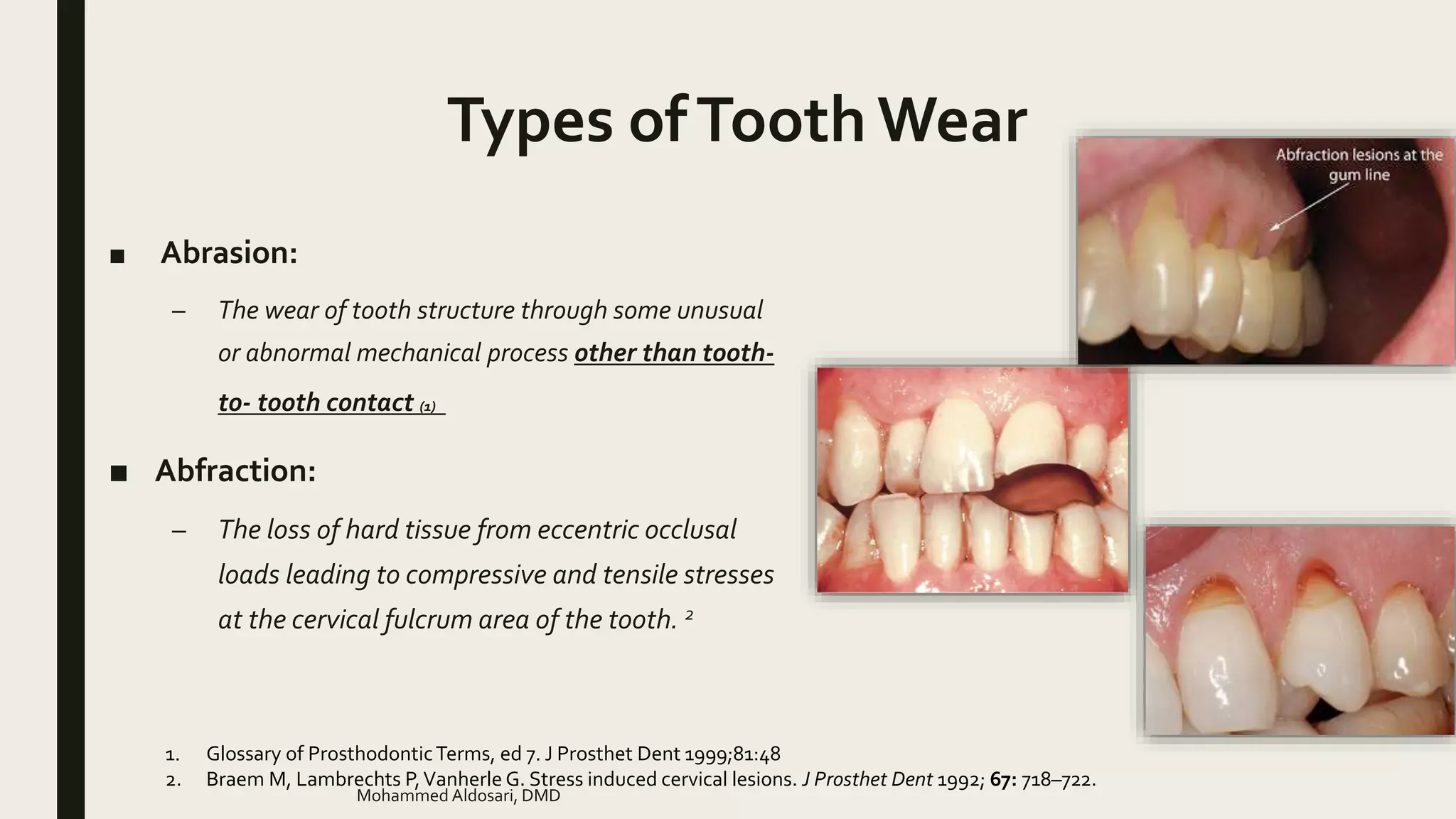
This document discusses tooth wear, including types, etiology, management, prevention, and restorative treatment. It defines tooth wear and describes the main types as attrition, erosion, abrasion, and abfraction. Factors that can increase tooth wear like amelogenesis imperfecta are also outlined. The document discusses consequences of tooth wear, classifications by Turner, and approaches to management including monitoring, preventative measures, restorations, and referrals. Treatment planning considerations and options for localized anterior tooth wear are also summarized.