Downloaded 58 times




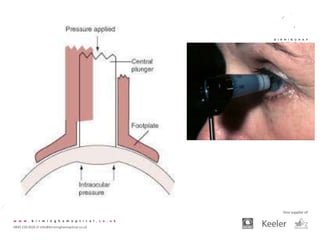
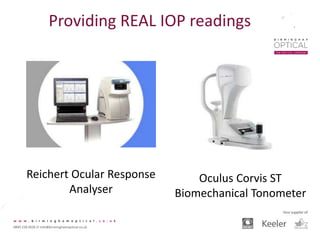
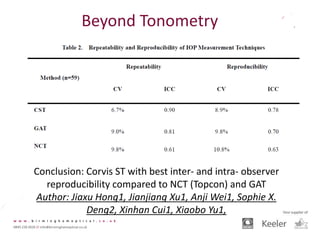
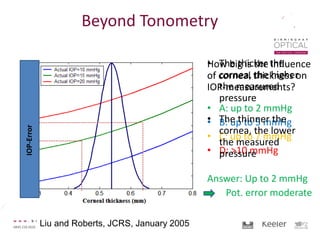
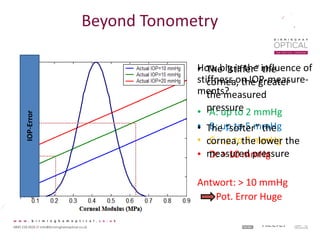
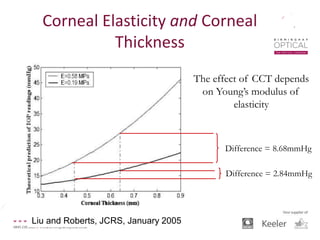
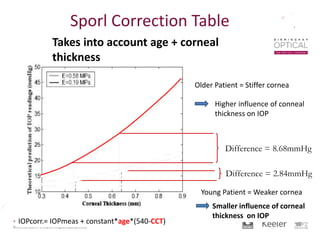

Tonometry, or the measurement of intraocular pressure (IOP), has evolved significantly over time. The Goldmann applanation tonometer, introduced in the 1950s, was long considered the gold standard but does not account for factors like corneal thickness and stiffness. Newer devices use air puffs, indentation, or advanced cameras to record the cornea's response and provide a more accurate IOP reading. Specifically, the Corvis ST uses a high-speed camera to measure hysteresis and account for biomechanical properties, allowing for a truly personalized IOP assessment. As technology advances, tonometry continues to improve our understanding and treatment of glaucoma.















































