Definition of tonguethrust
Classification
Etiology
Diagnosis
Treatment considerations
Case Reports
3.
What is TongueThrusting?
Tongue thrust is forward
movement of tongue tip
between the teeth to meet the
lower lip during deglutition and
in sounds of speech, so that the
tongue lies interdentally.
4.
1.
2.
3.
4.
Classification of TongueThrusting
Physiologic
Comprises of normal tongue thrust swallow of infancy
Habitual
Present as a habit even after correction of malocclusion
Functional
An adaptive behaviour developed to achieve oral seal
Anatomic
Person with enlarged tongue can have an anterior tongue
posture
5.
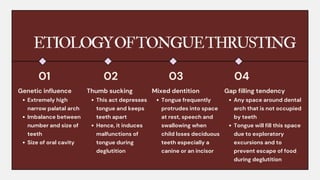
ETIOLOGYOFTONGUETHRUSTING
Genetic influence
Extremely high
narrowpalatal arch
Imbalance between
number and size of
teeth
Size of oral cavity
01 02 03 04
Thumb sucking
This act depresses
tongue and keeps
teeth apart
Hence, it induces
malfunctions of
tongue during
deglutition
Mixed dentition
Tongue frequently
protrudes into space
at rest, speech and
swallowing when
child loses deciduous
teeth especially a
canine or an incisor
Gap filling tendency
Any space around dental
arch that is not occupied
by teeth
Tongue will fill this space
due to exploratory
excursions and to
prevent escape of food
during deglutition
6.
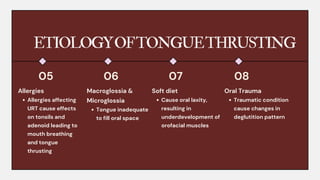
ETIOLOGYOFTONGUETHRUSTING
Allergies
Allergies affecting
URT causeeffects
on tonsils and
adenoid leading to
mouth breathing
and tongue
thrusting
05 06 07 08
Macroglossia &
Microglossia
Tongue inadequate
to fill oral space
Soft diet
Cause oral laxity,
resulting in
underdevelopment of
orofacial muscles
Oral Trauma
Traumatic condition
cause changes in
deglutition pattern
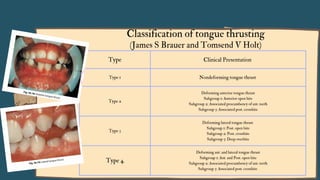
Type Clinical Presentation
Type1 Nondeforming tongue thrust
Type 2
Deforming anterior tongue thrust
Subgroup 1: Anterior open bite
Subgroup 2: Associated procumbency of ant. teeth
Subgroup 3: Associated post. crossbite
Type 3
Deforming lateral tongue thrust
Subgroup 1: Post. open bite
Subgroup 2: Post. crossbite
Subgroup 3: Deep overbite
Type 4
Deforming ant. and lateral tongue thrust
Subgroup 1: Ant. and Post. open bite
Subgroup 2: Associated procumbency of ant. teeth
Subgroup 3: Associated post. crossbite
Classification of tongue thrusting
(James S Brauer and Tomsend V Holt)
9.
1.
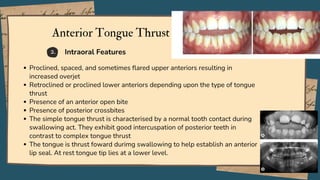
Anterior Tongue Thrust
Usuallydolichocephalic face
Increased lower anterior facial height
Incompetent lips
Expresionless face as the mandible is stabilized by facial muscles instead of
masticatory muscles during deglutition
Speech problems like sibiliant distortions and lisping
Abnormal mentalis muscle activity is seen
Extraoral Features
10.
Proclined, spaced, andsometimes flared upper anteriors resulting in
increased overjet
Retroclined or proclined lower anteriors depending upon the type of tongue
thrust
Presence of an anterior open bite
Presence of posterior crossbites
The simple tongue thrust is characterised by a normal tooth contact during
swallowing act. They exhibit good intercuspation of posterior teeth in
contrast to complex tongue thrust
The tongue is thrust foward durimg swallowing to help establish an anterior
lip seal. At rest tongue tip lies at a lower level.
2.
Anterior Tongue Thrust
Intraoral Features
11.
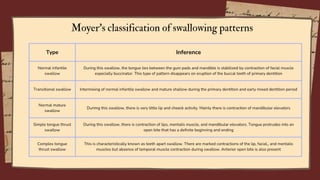
Type Inference
Normal infantile
swallow
Duringthis swallow, the tongue lies between the gum pads and mandible is stabilized by contraction of facial muscle
especially buccinator. This type of pattern disappears on eruption of the buccal teeth of primary dentition
Transitional swallow Intermixing of normal infantile swallow and mature shallow during the primary dentition and early mixed dentition period
Normal mature
swallow
Durimg this swallow, there is very little lip and cheeck activity. Mainly there is contraction of mandibular elevators
Simple tongue thrust
swallow
During this swallow, there is contraction of lips, mentalis muscle, and mandibular elevators. Tongue protrudes into an
open bite that has a definite beginning and ending
Complex tongue
thrust swallow
This is characteristically known as teeth apart swallow. There are marked contractions of the lip, facial,, and mentalis
muscles but absence of temporal muscle contraction during swallow. Anterior open bite is also present
Moyer’s classification of swallowing patterns
12.
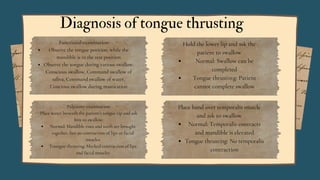
Diagnosis of tonguethrusting
Functional examination:
Observe the tongue position, while the
mandible is in the rest position
Observe the tongue during various swallow:
Conscious swallow, Command swallow of
saliva, Command swallow of water,
Concious swallow during mastication
Palpatory examination:
Place water beneath the patient’s tongue tip and ask
him to swallow:
Normal: Mandible rises and teeth are brought
together, but no contraction of lips or facial
muscles
Toungue thrusting: Marked contraction of lips
and facial muscles
Place hand over temporalis muscle
and ask to swallow
Normal: Temporalis contracts
and mandible is elevated
Tongue thrusting: No temporalis
contraction
Hold the lower lip and ask the
patient to swallow
Normal: Swallow can be
completed
Tongue thrustin:g: Patient
cannot complete swallow
13.
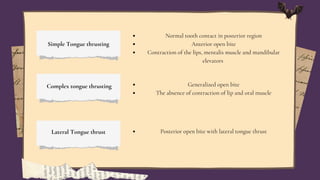
Simple Tongue thrusting
Normaltooth contact in posterior region
Anterior open bite
Contraction of the lips, mentalis muscle and mandibular
elevators
Complex tongue thrusting Generalized open bite
The absence of contraction of lip and oral muscle
Lateral Tongue thrust Posterior open bite with lateral tongue thrust
14.
Treatment considerations
Tongue thrustingoften self-corrects by 8-9
years of age by the time permanent teeth erupt.
But if the tongue thrusting is associated with other
habits, then the associated habit must be treated
first.
15.
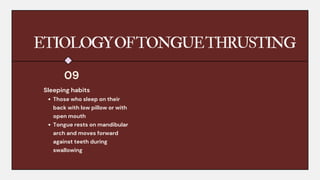
Myofunctional therapy
1.
This methodhelps to guide patient
regarding the correct posture of
the tongue during swallowing by
various kind of exercises like asking
the child to place the tip of tongue
in rugae area for 5 minutes and ask
the patient to swallow.
a specialized treatment used to correct tongue
thrust by retraining the muscles of the mouth
and face, focusing on improving tongue
posture, swallowing patterns, and oral function
through targeted exercises, aiming to establish
a proper resting tongue position against the
roof of the mouth instead of pushing forward
between the teeth
18.
2) orthodontic elastics
Thetongue tip is held
against the palate using
orthodontic elastic of
5/16" and sugarless fruit
drop
20.
3) lEMON CANDYEXERCISE
Instead of elastic, a lemon candy is put
on the tongue tip and patient is asked to
hold the candy against the palate by the
tongue tip and then asking the child to
swallow
21.
4) 2s exercise
2Sis refers to “spot” and “squeeze”
This is a myofunctional therapy includes
identifying the “spot” and then squeezing the
spot while keeping the tongue at the same
position
22.
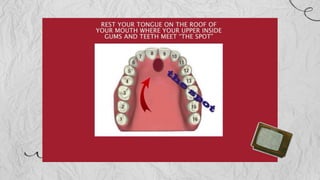
Place the tipof your tongue on the "spot" on
the roof of your mouth.
While maintaining tongue placement, gently
press your tongue against the palate, creating a
squeezing sensation.
Repeat this "spot and squeeze" action multiple
times throughout the day.
HOW TO PERFORM?
HOW TO PERFORM?
23.
5) 4s exercise
4Sstands for spot, salivate, squeeze, and swallow.
This includes identifying the spot, salivating,
squeezing the spot, and swallowing. Using the
tongue, the spot is identified, the tongue tip is
pressed against this spot, and the child is asked to
swallow keeping the tongue at the same spot.
25.
6) lip exercises
Tug-of-warand button pull exercise: A string is tied
to two buttons; one of the buttons is placed
between the lips of the patient while the other is
held by the patient outside. The outer button is
pulled outwards, and at the same time, the inside
button is resisting the forces, thereby strengthening
the lips on both aspects.
27.
7) other exercises
Thechild is asked to perform a
series of exercise such as
whistling, reciting the count from
60 to 69, gargling, yawning, etc.
to tone the respective muscles.
28.
8) Mechanotherapy
Both fixedand removable appliances can be
fabricated. The appliance re-educates tongue
so that the dorsum of tongue approximates
the palatal vault, and the tip of the tongue
contacts palatal rugae during deglutition.
29.
Some of theappliances that can be used to
prevent tongue thrusting are:
1) Pre-orthodontic trainer
2) Modifications of Hawley appliance
3) Tongue crib
4) Oral screen
30.
CASE REPORT :PRE-ORTHODONTIC TRAINER
Background: a 9-year-old boy diagnosed as Class II division 1
malocclusion with protruded upper anterior teeth, space loss in lower
arch and Class 2 molar relation on side.
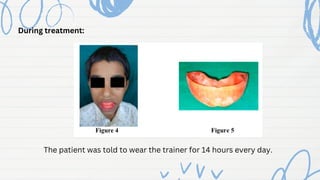
Treatment plan: Functional treatment approach was decided using pre
orthodontic T4K trainer for 12 months.
Correcting maxillary teeth’s proclination
1.
Relieve crowding of lower anterior teeth
2.
Enhance the arch shapes and tongue’s resting
position
3.
Establish the skeletal and molar class I relationship
4.
31.
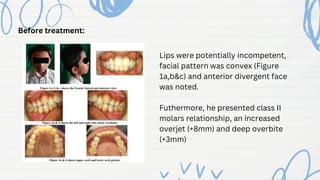
Before treatment:
Lips werepotentially incompetent,
facial pattern was convex (Figure
1a,b&c) and anterior divergent face
was noted.
Futhermore, he presented class II
molars relationship, an increased
overjet (+8mm) and deep overbite
(+3mm)
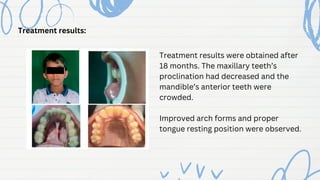
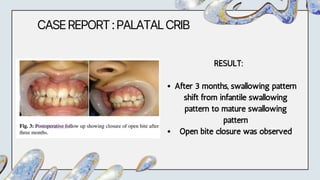
Treatment results:
Treatment resultswere obtained after
18 months. The maxillary teeth’s
proclination had decreased and the
mandible’s anterior teeth were
crowded.
Improved arch forms and proper
tongue resting position were observed.
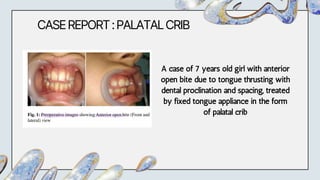
CASEREPORT:PALATALCRIB
A case of7 years old girl with anterior
open bite due to tongue thrusting with
dental proclination and spacing, treated
by fixed tongue appliance in the form
of palatal crib
36.
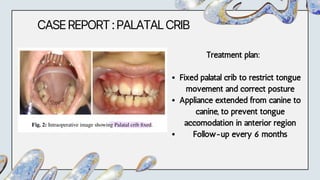
CASEREPORT:PALATALCRIB
Treatment plan:
Fixed palatalcrib to restrict tongue
movement and correct posture
Appliance extended from canine to
canine, to prevent tongue
accomodation in anterior region
Follow-up every 6 months
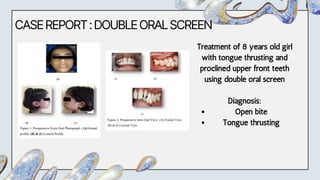
CASEREPORT:DOUBLEORALSCREEN
Treatment of 8years old girl
with tongue thrusting and
proclined upper front teeth
using double oral screen
Diagnosis:
Open bite
Tongue thrusting
39.
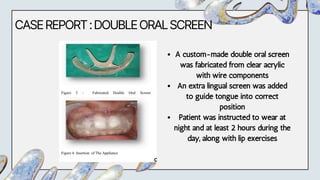
CASEREPORT:DOUBLEORALSCREEN
A custom-made doubleoral screen
was fabricated from clear acrylic
with wire components
An extra lingual screen was added
to guide tongue into correct
position
Patient was instructed to wear at
night and at least 2 hours during the
day, along with lip exercises
Case report: A7 year old girl reveals convex profile,
incompetent lip, retrusive chin and increased lower lip length
Presence of generalised marginal gingivitis, Angle’s class 1
malocclusion with open bite and presence of tongue thrusting
habit
42.
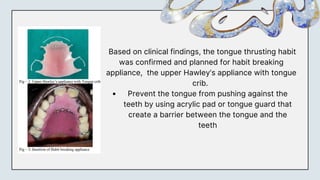
Based on clinicalfindings, the tongue thrusting habit
was confirmed and planned for habit breaking
appliance, the upper Hawley’s appliance with tongue
crib.
Prevent the tongue from pushing against the
teeth by using acrylic pad or tongue guard that
create a barrier between the tongue and the
teeth
43.
Dr. Priyanka Soakar.(2019, May 8). Tongue Thrusting.
https://bestorthodontistbracespune.in/DeccanDentalBlog/2019/05/08/tongue-thrusting/
1.
Guide to tongue thrust exercises. (2024, March 1). https://healthandfitness11.com/guide-to-tongue-thrust-exercises/
2.
Bansal, Karan, et al. “Treating the Tongue Thrusting: A Case Report.” IP Indian Journal of Orthodontics and
Dentofacial Research, vol. 6, no. 3, 15 Sept. 2020, pp. 181–183, https://doi.org/10.18231/j.ijodr.2020.035. Accessed 7 Aug.
2021.
3.
Das, Dr Abhishek, et al. “Treatment of Proclined Anterior Teeth with Tongue Thrusting Habit Using Double Oral Screen:
A Case Report.” International Journal of Dental Science and Innovative Research, vol. 2, no. 5, 2019, pp. 437–440,
www.ijdsir.com/asset/images/uploads/15728819794824.pdf.
4.
Nikhil Marwah. Textbook of Pediatric Dentistry. New Delhi, India, Jaypee Brothers Medical Publishers (P) Ltd, 2019.
5.
Ramesh, et al. “A case report: Pre-orthodontic trainer in 9-year-old child” International Journal of Pedodontic
Rehabilitation, 1 January 2023, https://www.researchgate.net/publication/368229566_Case_report_on_pre-
orthodontic_trainer_in_a_9-year-
old_child_with_12_months_follow_up_Case_Report/fulltext/63dd242564fc8606381358c5/Case-report-on-pre-
orthodontic-trainer-in-a-9-year-old-child-with-12-months-follow-up-Case-Report.pdf?
origin=publication_detail&_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0a
W9uRG93bmxvYWQiLCJwcmV2aW91c1BhZ2UiOiJwdWJsaWNhdGlvbiJ9fQ
6.
References















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



