Downloaded 25 times
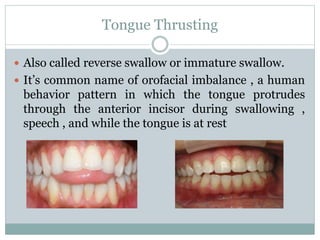
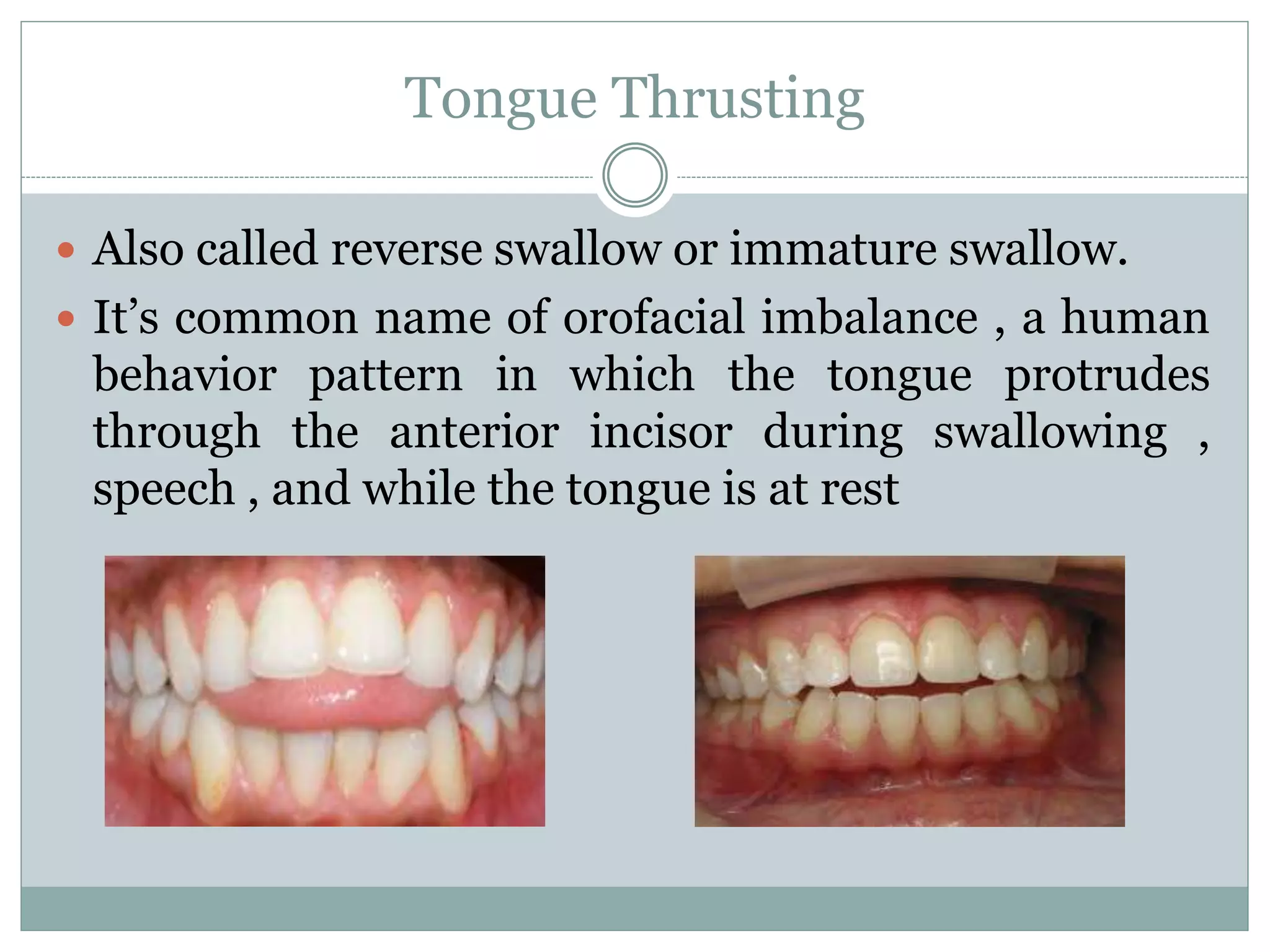
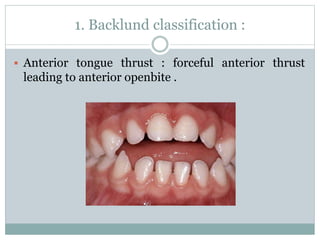
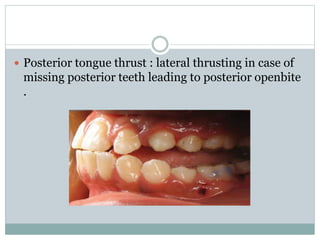

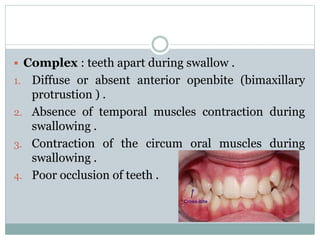
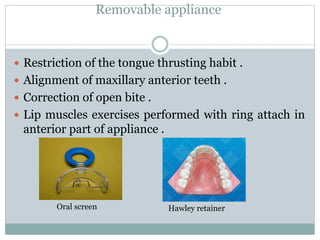


This document summarizes information about tongue thrusting, including its causes, characteristics, classifications, and treatment. Tongue thrusting is when the tongue protrudes through the front teeth during swallowing, speech, and at rest. It is common in children and can be caused by factors like retained infantile swallow reflex, mouth breathing, neurological issues, or feeding practices. Tongue thrusting can lead to malocclusion and is classified in different ways, including by whether it involves anterior or posterior thrusting. Treatment involves training correct swallowing and tongue posture, speech therapy, appliances to guide the tongue, and orthodontics if needed.













































































