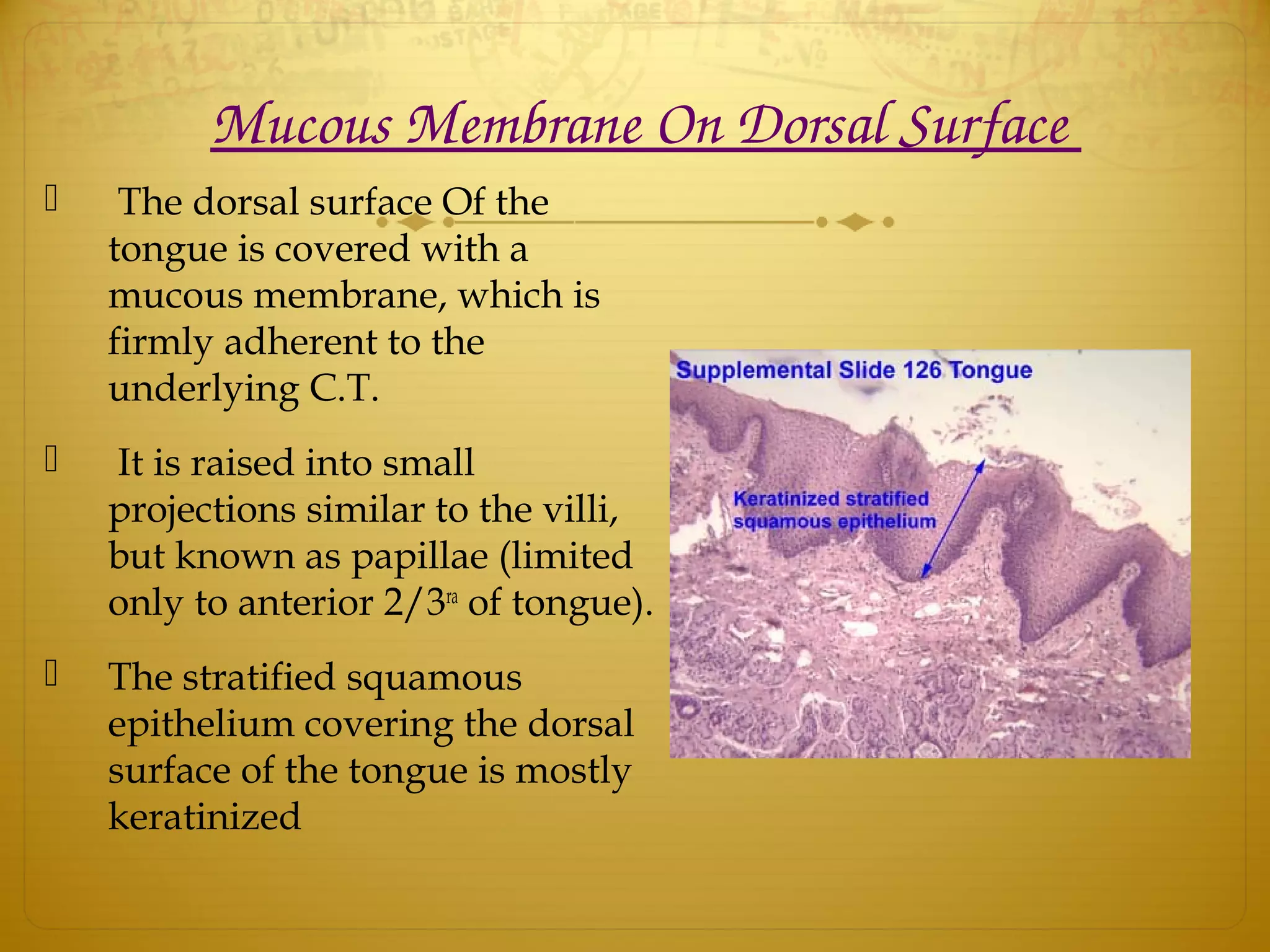
This document provides an overview of the anatomy and histology of the tongue. It discusses the parts and surfaces of the tongue, the intrinsic and extrinsic muscles, vascular supply, innervation, and histology. It also covers clinical considerations such as injuries, diseases, and malignant tumors that can affect the tongue.