
Downloaded 34 times



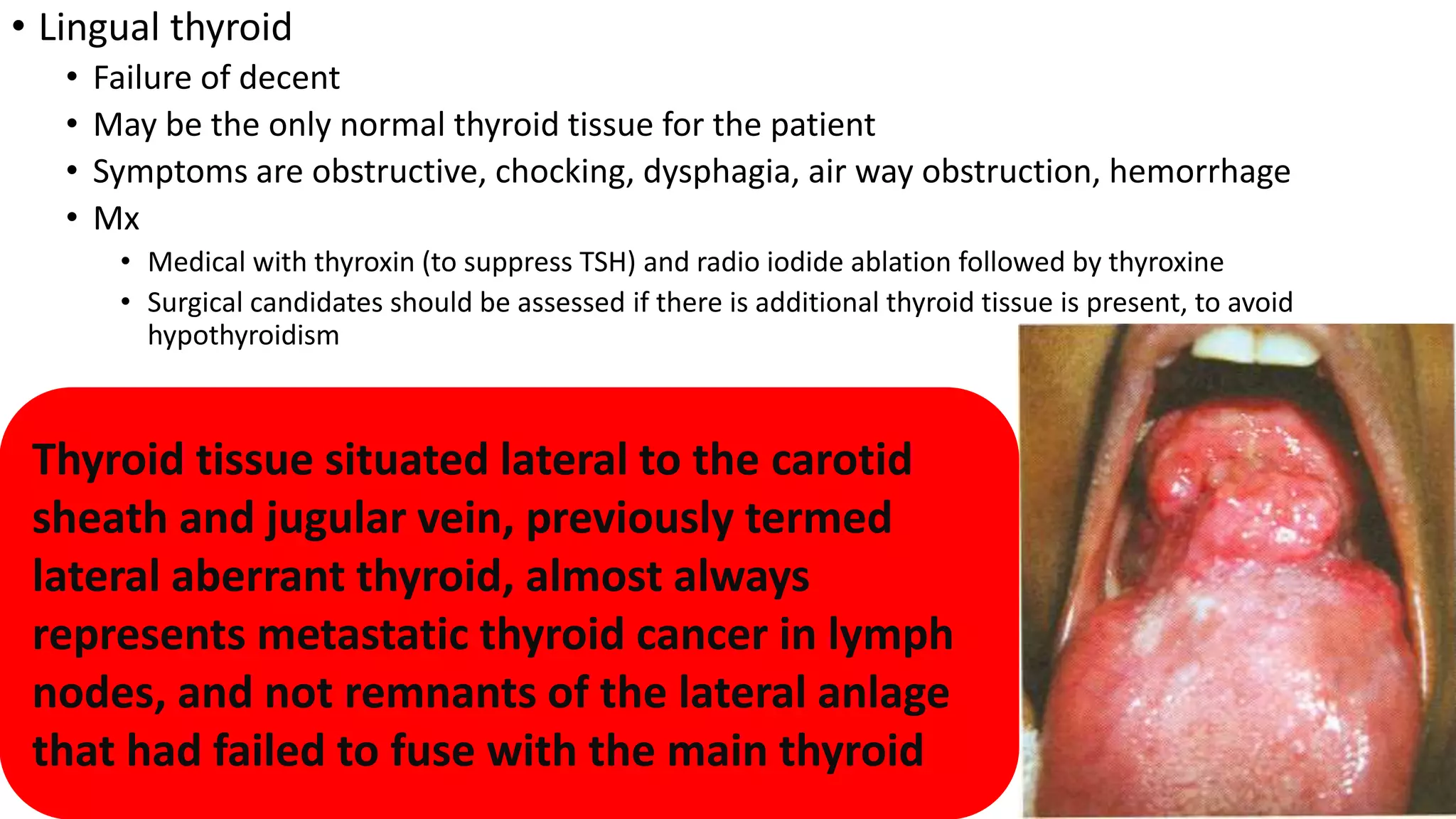













The thyroid gland develops from endodermal thickening in the floor of the mouth and descends to its final location in the neck. It normally forms by week 7 and contains two lobes connected by an isthmus. Congenital abnormalities can include thyroglossal cysts or lingual thyroid. The thyroid produces T4 and T3 hormones which regulate metabolism. Hyperthyroidism includes Graves' disease, while hypothyroidism is often Hashimoto's thyroiditis. Treatment involves restoring normal thyroid levels through medication.



































































