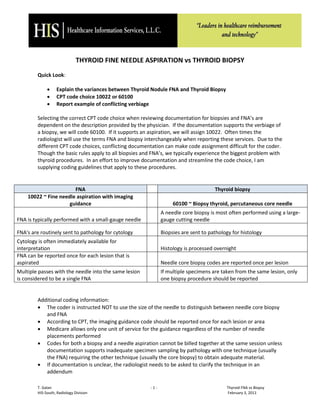
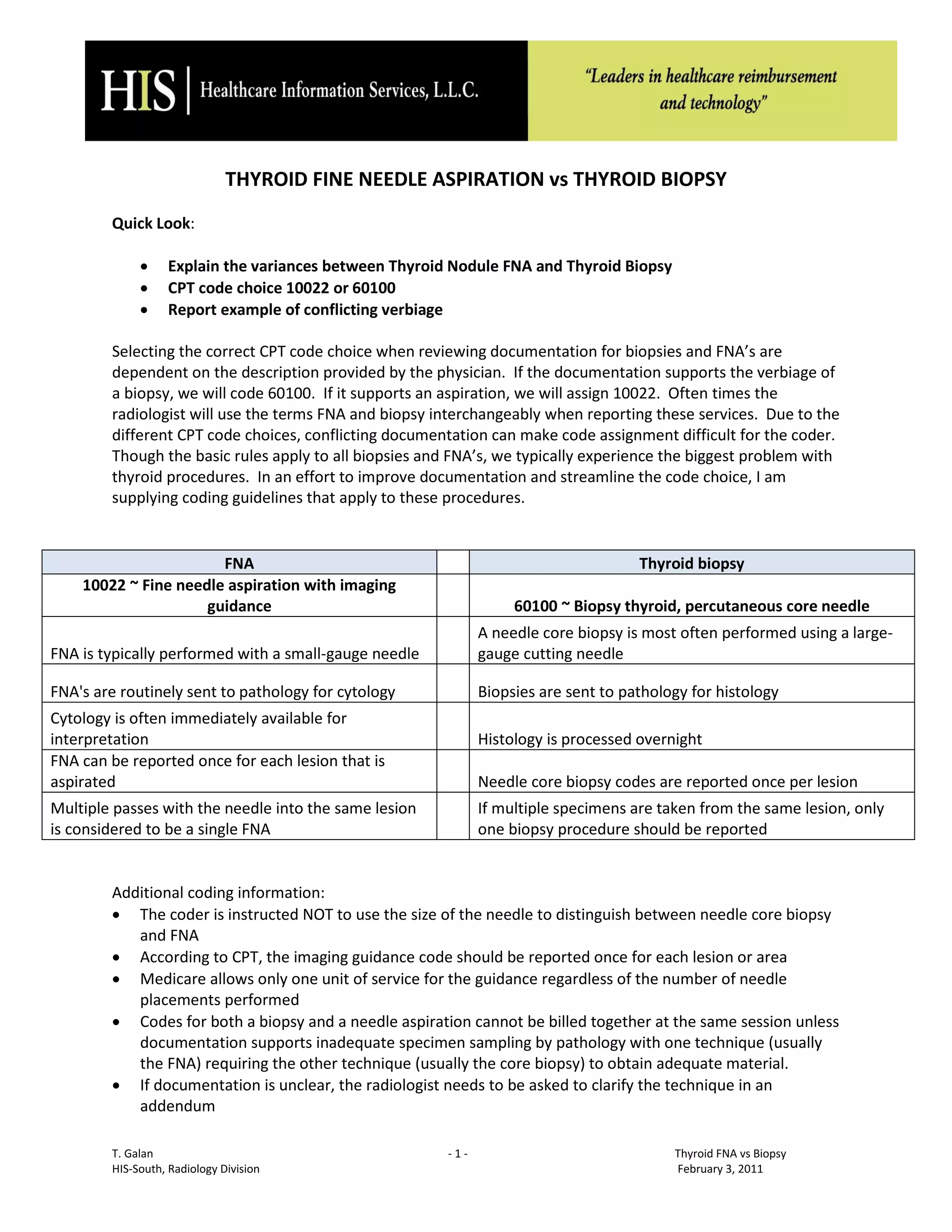
The document outlines the differences between thyroid fine needle aspiration (FNA) and thyroid biopsy, detailing the appropriate CPT code selection based on physician documentation. It emphasizes the importance of clear terminology to prevent coding confusion and provides specific guidelines for coding these procedures. Additionally, it discusses a case example of ultrasound-guided thyroid biopsy to illustrate proper documentation and coding practices.






![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)






















































![FNAC_DIRECT_and_GUIDED Pathology [1]_FINAL2.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fnacdirectandguided1final2-260109235635-59e75d7d-thumbnail.jpg?width=640&height=640&fit=bounds)





![BIOPSY IN SURGERY 1 [Auto-savedd] 3.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/biopsyinsurgery1auto-saved3-251018145913-707215d9-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















