Download as PDF, PPTX




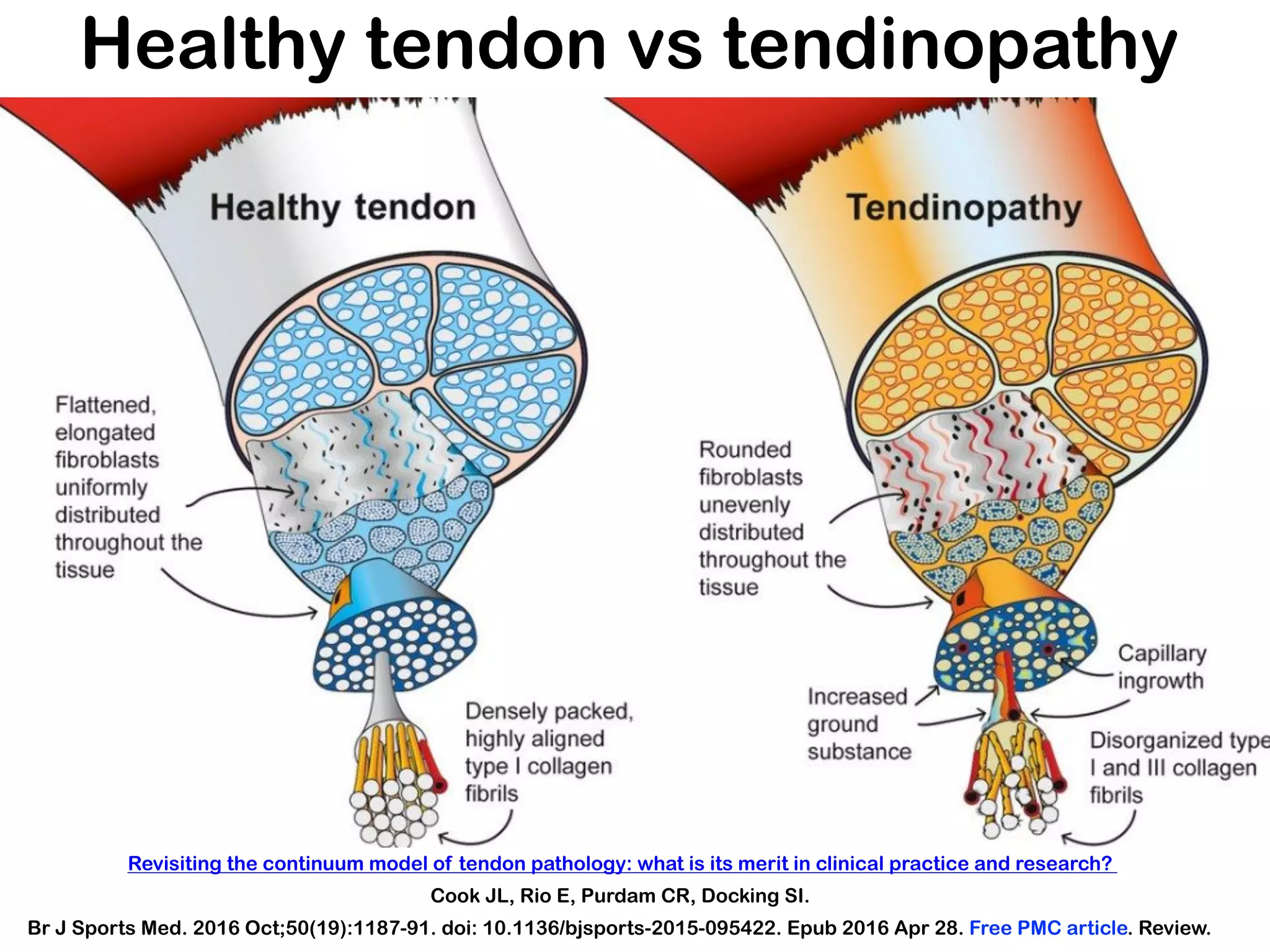



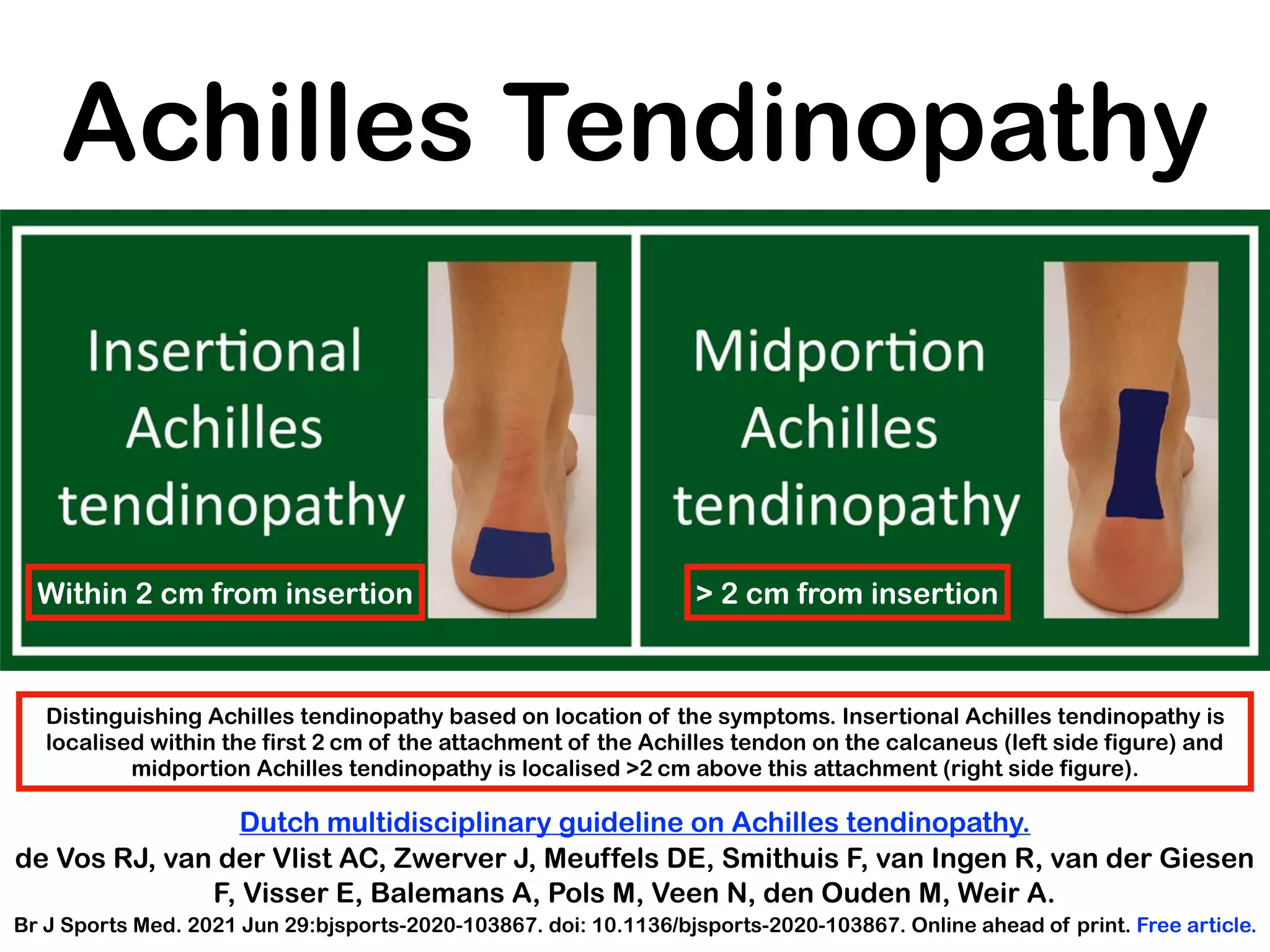


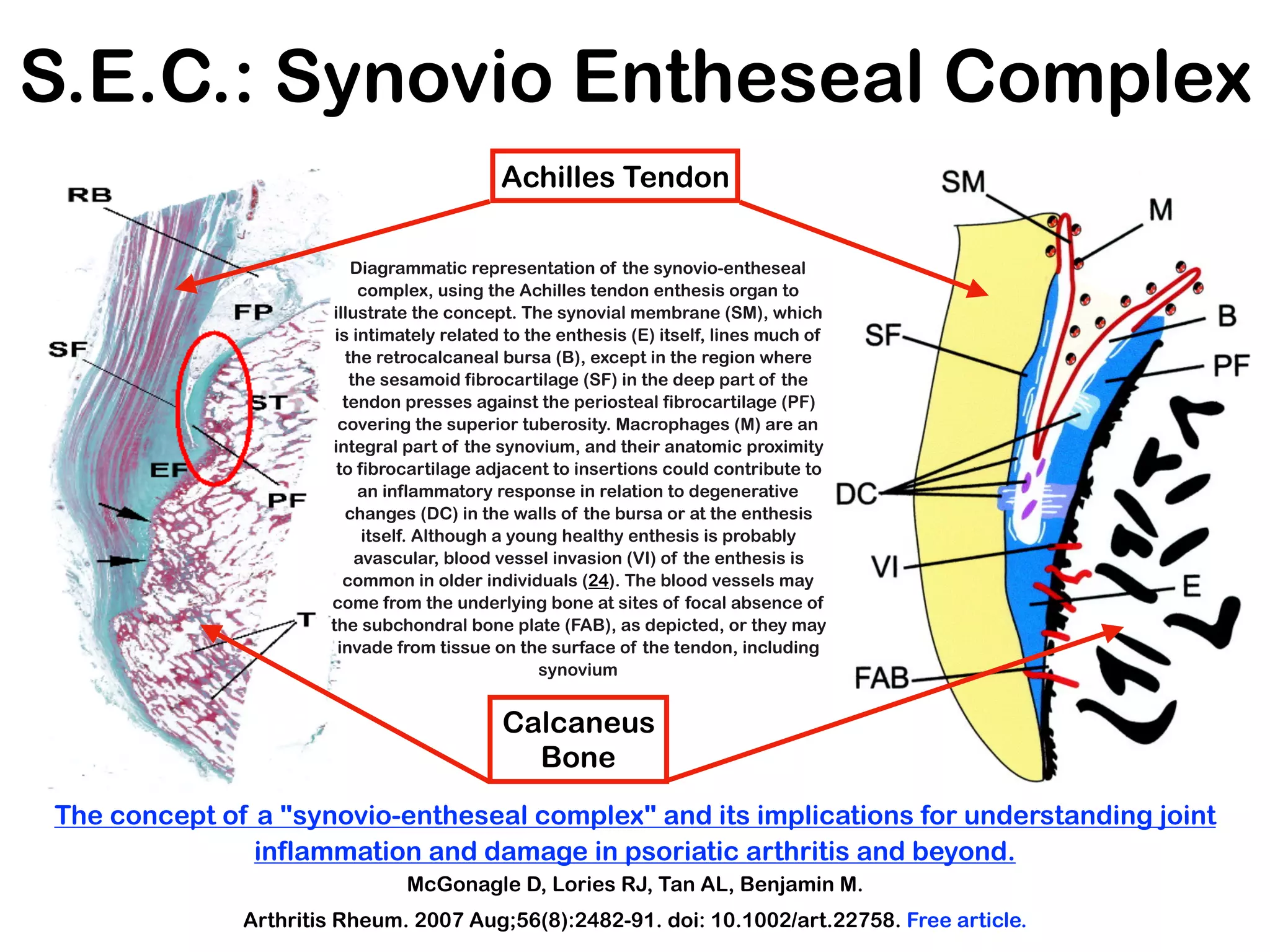
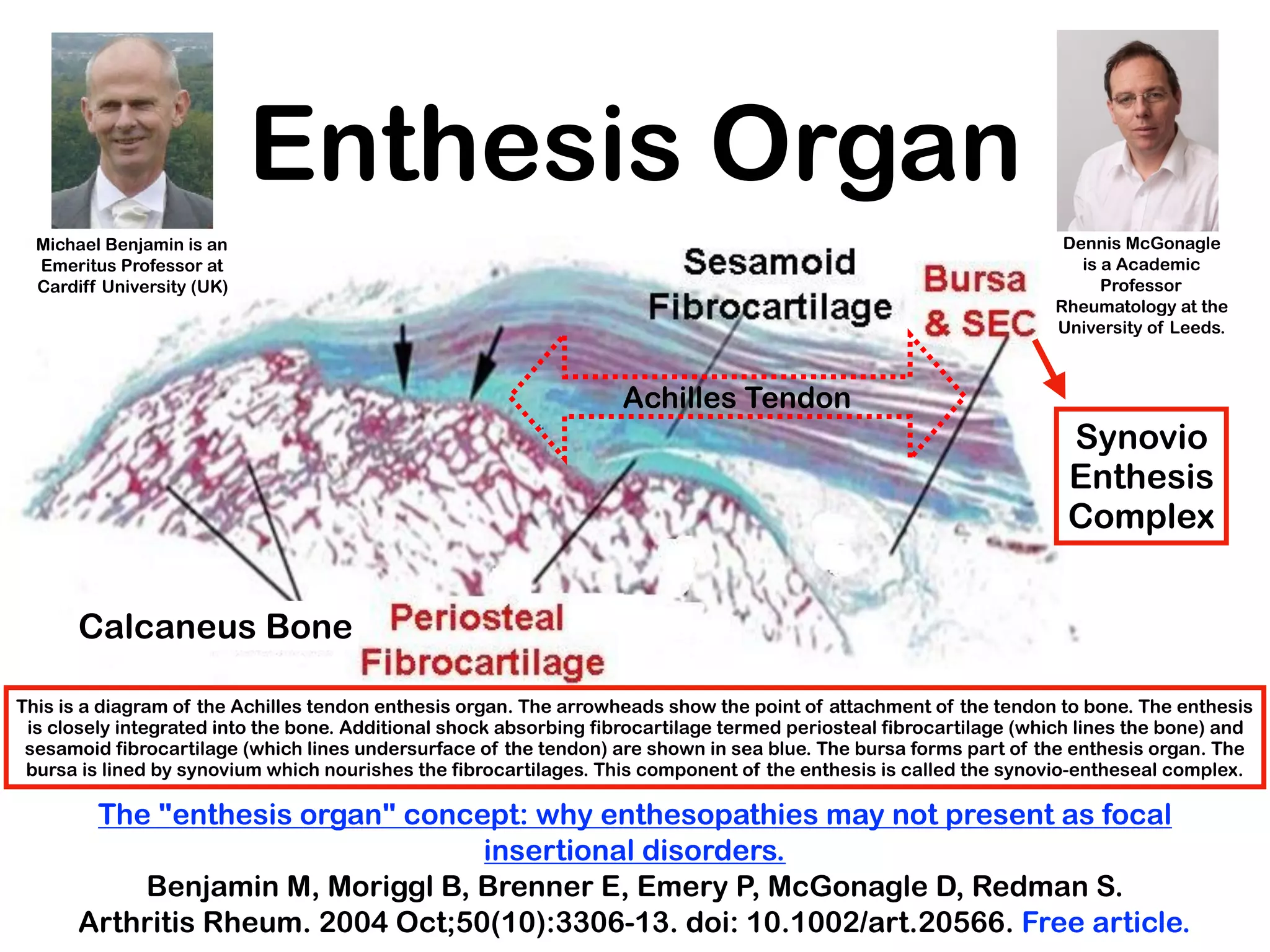























The VII International Congress on Sport Traumatology, held on December 11-12, 2020, explored advancements in understanding and treating sport-related injuries, particularly focusing on tendinopathies. Experts from various fields, including sports medicine and rehabilitation, presented evidence-based insights on conditions like Achilles tendinopathy and the role of fat pads in tendon health. The congress aimed to enhance knowledge and treatment approaches in sports medicine through collaborative discussions among professionals worldwide.









![Cassie and heathers powerpoint[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cassieandheatherspowerpoint1-101124095231-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




































































