Downloaded 21 times
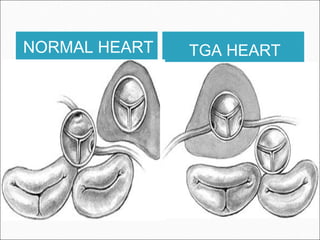
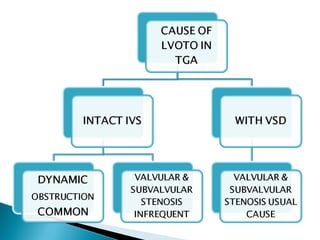
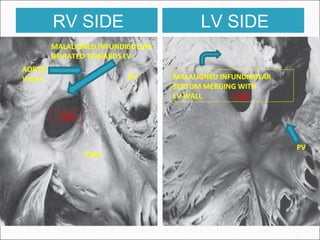
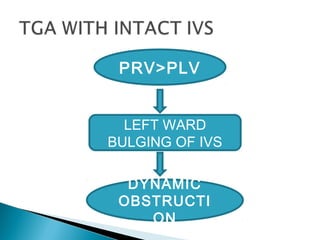
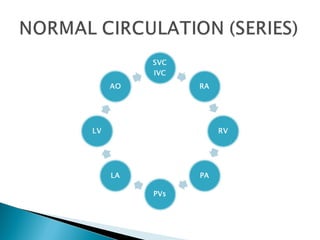
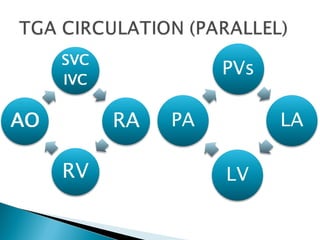


This document discusses the anatomy, pathophysiology, and clinical presentation of transposition of the great arteries (TGA). Key points include: - In TGA, the aorta arises from the right ventricle and the pulmonary artery arises from the left ventricle, compared to the normal arrangement. This results in deoxygenated and oxygenated blood mixing through a ventricular septal defect or patent ductus arteriosus. - Survival without treatment is poor, particularly for those with an intact ventricular septum. Common associated anomalies include ventricular septal defects. Long term complications include pulmonary vascular disease and left ventricular outflow tract obstruction. - The document provides detailed descriptions of the anatomical variations and abnormalities






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












