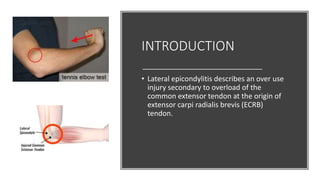
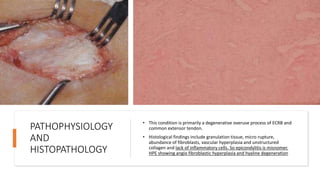
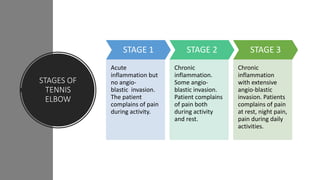
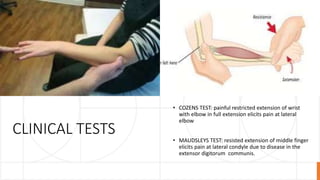
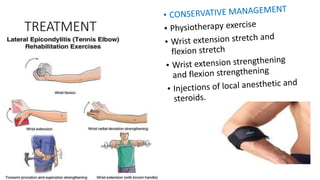
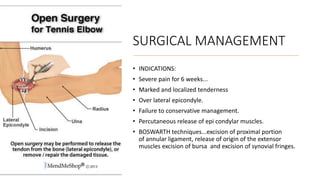
This document provides an overview of tennis elbow (lateral epicondylitis). It describes tennis elbow as an overuse injury of the forearm muscles originating at the lateral epicondyle of the elbow. Common causes are repetitive gripping and wrist extension motions from activities like tennis. Symptoms include pain over the lateral elbow that is worsened by resisted wrist extension. Conservative treatments include bracing, ultrasound therapy, and corticosteroid injections. Surgery is considered if conservative treatments fail after 6 weeks and for those with persistent, severe pain. The document covers evaluation, differential diagnosis, stages of the condition, clinical tests, imaging findings, and various treatment approaches for tennis elbow.