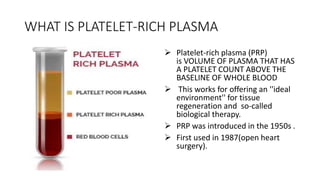
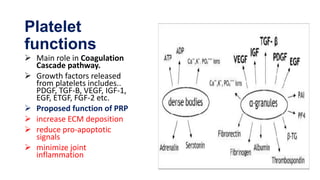
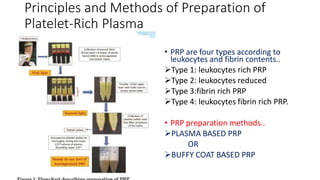
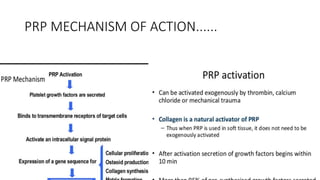
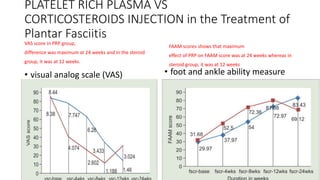
This document discusses platelet-rich plasma (PRP), which contains a higher concentration of platelets than normal blood. PRP was first used in the 1950s and releases growth factors that can promote tissue regeneration. There are different types of PRP classified by their leukocyte and fibrin contents. PRP is prepared either through plasma-based or buffy coat-based methods. Current clinical applications of PRP include treatment of osteoarthritis, tendonitis, and plantar fasciitis. A study found PRP more effectively reduced pain and improved foot function over 24 weeks compared to corticosteroid injections, which were most effective at 12 weeks.