1. A 35-year old male with type 1 diabetes was admitted with fever, cough, and breathlessness due to right lower lobe pneumonia.
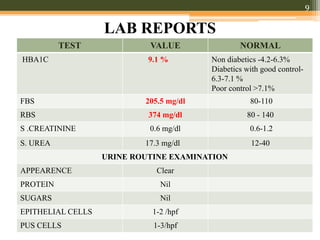
2. Laboratory tests showed elevated HbA1c of 9.1% and fasting blood sugar of 205.5 mg/dl. Chest x-ray found right lower lobe lung consolidation.
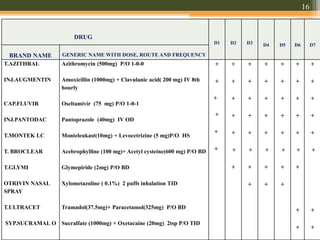
3. He was treated with antibiotics, cough suppressants, diabetes medications, and inhalers. His symptoms improved and he was discharged on oral medications with instructions to follow up in one week.

![23.
1. Elevated HbA1C[9.1%]
2. Elevated fasting blood sugar [ 205.5 mg/dl]
3. X ray showed right lower lobe consolidation of lung.
4. Smear for gram stain in sputum identified occasional gram
negative bacilli and few gram positive cocci .](https://image.slidesharecdn.com/type1dmabel-190708071040/85/Case-Presentation-in-SOAP-Format-23-320.jpg)





















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














