
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hypertensive emergencies
Similar to Hypertensive emergencies (20)
More from Myiesha Taylor
Recently uploaded
Recently uploaded (20)
Hypertensive emergencies
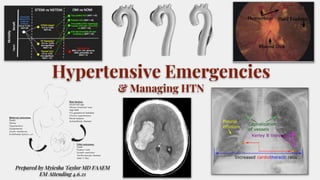
- 1. Hypertensive Emergencies & Managing HTN Prepared by Myiesha Taylor MD FAAEM EM Attending 4.6.21
- 2. A 47-year-old African American male presents to the ED complaining of a laceration to his finger he sustained while cooking. His tetanus is up to date, the bleeding is controlled, and you successfully repair the uncomplicated laceration. Prior to discharge, you review the patient’s vital signs and find a blood pressure of 190/115. The patient has no complaints. What needs to be done about this elevated blood pressure? The Case Vignette:
- 3. Is this a Hypertensive EMERGENCY or Urgency?
- 4. Hypertensive Urgency (severe asymptomatic HTN) Minimally or asymptomatic patients without evidence of end organ damage with markedly elevated blood pressure ● typically >180s/110s ● They may present with headache, shortness of breath, epistaxis, or anxiety but often are asymptomatic.*
- 5. Hypertensive Emergency Definition: end-organ damage due to hypertension Blood pressure is generally >180/120 (usually > 220/130), but presence of end-organ damage defines disease (not absolute blood pressure number) Is rare Elevated blood pressure with evidence of end-organ damage. Heart - acute coronary syndrome and myocardial infarction Aortic - dissection Renal - evidence of worsening functioning or failure Pulmonary - edema Neurological - mental status changes (encephalopathy) or evidence of stroke (infarction or bleeding) Pregnancy - eclampsia
- 6. Hypertensive Emergency Not based on a number!! It is based on evidence of END ORGAN DAMAGE!!
- 7. Malignant Hypertension A patient with malignant hypertension always has retinal papilledema (as seen in the image below), as well as flame-shaped hemorrhages and exudates. Other clinical features of malignant hypertension may include encephalopathy, confusion, left ventricular failure, intravascular coagulation, and impaired renal function, with hematuria and weight loss. The pathologic hallmark of malignant hypertension is fibrinoid necrosis of the arterioles, which occurs systemically, but specifically in the kidneys. These patients develop fatal complications if untreated, and more than 90% will not survive beyond 1-2 years. - always has papilledema, hemorrhages/exudates
- 8. Indicators of End-Organ Damage Altered mental status - seizures, infarction, intracranial hemorrhage, encephalopathy Shortness of breath - congestive heart failure Chest pain - acute myocardial infarction, EKG changes Neurologic deficit - aortic dissection (can present as neurologic deficit, chest pain, or back pain); stroke Ophthalmologic - vision changes, retinal changes/hemorrhages, exudates, and papilledema Diminished kidney function - oliguria, elevated serum creatine, UA evidence of kidney damage
- 9. Pertinent History & Focused Physical Exam Double check the BP (ensure proper cuff size, check both extremities, take multiple readings with the patient calm) BP discrepancy in the upper extremities could indicate aortic dissection Past medical history of high-risk conditions? Medication history and compliance. Social History - drug use (both illicit such as cocaine and methamphetamines, and OTC such as sympathomimetic medications. Acute stressors. Fundoscopic exam and visual fields Chest exam - evidence of pulmonary edema Extremity exam - evidence of edema (CHF) Abdominal masses (aortic disease)
- 10. Diagnostic Testing ● Clinical judgement and risk-factors inform the decision of necessary work-up. If risk-factors, concerning historical points, or physical exam findings suggest possible end organ damage, further evaluation is appropriate. ○ Renal - UA (proteinuria/hematuria/cells/casts), CMP ○ Vascular - CBC with peripheral smear to r/o microangiopathic anemia. Aortic ultrasound or CT scan of the chest/abdomen/pelvis. ○ Cardiopulmonary - EKG, CXR, cardiac enzymes, BNP, ECHO ○ Neuro - Head CT ○ Beta HCG - rule-out pregnancy ○ Utox ○ Endocrine considerations - Thyroid & parathyroid disease, pheochromocytoma, mineralocorticoid excess, Cushing disease, SLE, pregnancy) * isolated HA does not warrant a HCT as this has not been shown to be a risk factor for end-organ CNS damage. “a headache is not a hypertensive emergency unless the patient looks so bad that you are rushing her to CT”
- 11. Treatment for HTN Urgency Rapidly lowering blood pressure in the emergency department is usually unnecessary in asymptomatic patients and may be harmful. Reducing severely elevated blood pressure below the autoregulatory zone too quickly can result in markedly decreased perfusion to the brain and eventually ischemia or infarction. Outpatient treatment is generally acceptable, with appropriate follow-up. If it is unclear whether the patient will comply with follow- up, a short hospital stay may be needed. Initiating treatment for asymptomatic hypertension is optional with appropriate follow-up. Tx in ischemic strokes (and if the provider lowers the BP too aggressively precipitating a stroke): The problem with ischemic strokes is they will generally have an ischemic penumbra surrounding the core of the stroke. This is an area that’s at risk for death; thus, having an elevated blood pressure is beneficial at minimizing the stroke size through collateral circulation.
- 13. Treatment of HTN EMERGENCY Admit adults with a hypertensive emergency to an ICU for continuous monitoring of BP and target organ damage, as well as for parenteral administration of an appropriate medication. For adults with a compelling condition (aortic dissection, severe preeclampsia/eclampsia, or pheochromocytoma crisis), lower SBP to below 140 mm Hg during the first hour and to below 120 mm Hg in aortic dissection. For adults without a compelling condition, reduce the SBP to a maximum of 25% within the first hour; then, if the patient is clinically stable, lower the BP to 160/100 -110 mm Hg over the next 2-6 hours, and then cautiously to normal over the following 24-48 hours.
- 15. Treatment of HTN EMERGENCY - the drugs 1. B-blockers: Labetolol is useful for most hypertensive emergencies (preferred in aortic dissection and ESRD). Give a 20mg slow IV push, then double the dose q10 min, up to 300mg. Be cautious in patients with asthma or COPD, and hepatic failure. Esmolol has quicker onset/offset, and may be safer in patients with mildly reactive airways. 2. Vasodilators: Nitroglycerin is great for ACS and pulmonary edema, but arterio-dilates only at high doses. Therefore for CHF patients, use higher doses to produce afterload reduction. Nitroprusside dilates both arteries and veins, but generates cyanide w/ prolonged use of high doses as it breaks down. Starting dose is 0.3–0.5mcg/min, and max dose is 2 mcg/min (less in renal pts). Hydralazine also dilates arteries, but has less predictable effects, and raises HR. Phentolamine (an a1 blocker) arterio-dilates to counteract catecholamines (i.e. cocaine, pheochromocytoma). 3. Calcium channel blockers: Dihydropyridine CCBs lower blood pressure by vasodilation (amlodipine, nifedipine, and nicardipine). The phenylalkylamine class of CCBs mainly have negative inotropic and negative chronotropic effects (diltiazem and verapamil). Clevidipine, a dihydropyridine CCB, is administered IV for rapid and precise BP reduction. [25] It is rapidly metabolized in the blood and tissues and does not accumulate in the body. Initiate IV infusion of clevidipine at 1-2 mg/hour; titrate the dose at short intervals (ie, 90 seconds) initially by doubling the dose. Parenteral (IV): ● Labetalol ● Esmolol ● Nitroglycerin ● Nitroprusside ● Nicardipine ● Clevidipine ● Fenoldopam ● Hydralazine
- 17. Treatment of HTN EMERGENCY **Use the drug you are most familiar with, if the clinical context is appropriate. Aortic dissection: labetalol or esmolol. Followed by vasodilator. If contraindications to b-blocker, do diltiazem. Congestive Heart Failure (CHF): high dose nitroglycerin to achieve arterial dilatation. Give up to 6 sublingual doses while IV drip is being prepared. Non-invasive positive pressure. BP can be very high, so verify and monitor by an arterial line in the right radial artery. Pre-eclampsia is BP >160 /110, along with proteinuria (or low platelets, elevated LFT or Cr) or pulmonary, liver, cerebral or visual symptoms, in a patient >20 weeks pregnant. Moms LoveHealthyNewborns: Use Methyldopa, Labetalol, Hydralazine, or Nifedipine for hypertensive pregnant women. Eclampsia is the same, but with seizures. Labetalol plus Mg+, although hydralazine (5mg IV slow push over 1-2 minutes, repeat 5-10mg prn) can be used as a second line. Give 2g/hr IV Mg+ for seizure prophylaxis. *Goal is still only 25% BP reduction, and consult OB as delivery is the definitive treatment
- 18. The drugs - when and how Cardiovascular emergencies - labetalol, nicardipine, nitroprusside (with beta-blocker), esmolol, and morphine sulfate. Rapid BP reduction is also indicated in cardiovascular emergencies, such as aortic dissection, acute coronary syndrome, and acute heart failure. Beta blockers are the recommended antihypertensive agents in patients with hypertension and thoracic aortic disease. However, avoid beta-blockers if there is aortic valvular regurgitation or suspected cardiac tamponade. Rapidly lower the SBP to below 120 mm Hg. Beta blockade should precede vasodilator administration, if needed for BP control or to prevent reflex tachycardia. Maintain the SBP below 110 mm Hg, unless signs of end-organ hypoperfusion are present. The preferred treatment includes a combination of narcotic analgesics (morphine sulfate), beta blockers (labetalol, esmolol), and vasodilators (nicardipine, nitroprusside). CCBs (verapamil, diltiazem) are an alternative to beta blockers. Hypertensive encephalopathy - reduce the MAP 25% over 8 hours. Labetalol, nicardipine, esmolol are the preferred medications; nitroprusside and hydralazine should be avoided. Acute ischemic stroke - labetalol and nicardipine. Withhold antihypertensive medications unless the SBP is above 220 mm Hg or the DBP is over 120 mm Hg, unless patient is getting tPA. For acute coronary syndrome - beta blockers and nitroglycerin are the preferred drugs. Reduce the BP by 20%-30% of baseline. Note that thrombolytics are contraindicated if the BP is above 185/100 mm Hg. Be careful with nitrates and Viagra-type drugs on board. In acute heart failure, the preferred medications are IV nitroglycerin or sublingual nitroglycerin and IV enalapril. In hypertensive adults with reduced ejection fraction (HFrEF) nondihydropyridine CCBs (verapamil, fendiline, diltiazem) are not recommended for treatment in this patient population. Acute intracerebral hemorrhage - the preferred medications are labetalol, nicardipine, and esmolol; avoid nitroprusside and hydralazine. The treatment is based on clinical/radiographic evidence of increased intracranial pressure (ICP). If there are signs of increased ICP, maintain the MAP just below 130 mm Hg (or SBP < 180 mm Hg) for the first 24 hours after onset. Cocaine toxicity/pheochromocytoma - Diazepam, phentolamine, and nitroglycerin/nitroprusside are the preferred drugs. However, avoid beta-adrenergic antagonists before administering phentolamine. Hypertension and tachycardia from cocaine toxicity rarely require specific treatment. Alpha-adrenergic antagonists (phentolamine) are the preferred agents for cocaine-associated acute coronary syndromes. Pheochromocytoma treatment guidelines are similar to that of cocaine toxicity.
- 19. Use the Mean Arterial Pressure to guide your treatment MAP is what the automated BP cuff is actually measuring. MAP may be most closely related to the risk of hypertensive emergency. MAP is preferred in guiding therapy. The best way to titrate antihypertensive drugs in a logical fashion is to target a specific MAP.
- 20. Take home points regarding HTN Urgency/Emergency Hypertensive urgency is an acute, severe elevation in blood pressure without signs or symptoms of end-organ damage. Proposed blood pressure levels indicating hypertensive urgency are arbitrary and not associated with short-term morbidity and mortality. Hypertensive urgency is common in the outpatient setting. In the absence of symptoms of target organ damage, most patients can be safely treated in the outpatient setting. Referral to the ED was associated with increased use of health care resources but not better outcomes. Focus on symptoms of end-organ damage in the patient's history, including chest pain, shortness of breath, headache, neurologic deficits, and vision changes. If a maintenance dose of an oral antihypertensive is initiated, the patient may be sent home without waiting for normalization of blood pressure. Over weeks to months, the dosage and selection of medications may be modified to achieve desired goals. Caution is advised in pregnant patients with hypertension. Preeclampsia can ensue at lower blood pressure levels than expected in other hypertensive emergencies. Treat the patient, not the number. Rapidly bringing down blood pressure in a patient without end-organ damage may result in relative hypoperfusion and harm the patient rather than help. In patients with asymptomatic markedly elevated blood pressure, routine ED medical intervention is not required. Patients with asymptomatic markedly elevated blood pressure should be referred for outpatient follow-up.
- 22. Case Resolution The patient reports he has been told in the past he has had high blood pressure by his doctor, but has not seen by his primary care provider (PCP) in over one year. You discuss with the patient the need for the patient to follow up with his doctor for repeat blood pressure measurement and give appropriate discharge instructions regarding both wound care and elevated blood pressure. The patient returns ten days later for suture removal and reports he has seen his doctor and was started on medication for his hypertension.
Editor's Notes
- Photos: ICH https://en.wikipedia.org/wiki/Hypertensive_emergency Eye findings: https://slidetodoc.com/hypertensive-emergencies-trevor-langhan-pgy3-november-10-2005/ CHF: https://glassboxmedicine.com/2019/03/23/radiology-abnormal-chest-x-rays-part-ii/ OMI, NOMI, STEMI, NSTEMI https://emcrit.org/emcrit/omi-manifesto/ Aorta: https://www.urmc.rochester.edu/MediaLibraries/URMCMedia/critical-care-nursing-symposium/documents/Hypertensive-Crisis.pdf Pre-eclampsia: https://www.google.com/url?sa=i&url=https%3A%2F%2Fjournals.physiology.org%2Fdoi%2F10.1152%2Fphysiolgenomics.00125.2015&psig=AOvVaw1GCNQA4y6lHSzwt7ZlU92y&ust=1617838633534000&source=images&cd=vfe&ved=0CAMQjB1qFwoTCIDf9d3k6u8CFQAAAAAdAAAAABAL
- Case: https://rebelem.com/elevated-asymptomatic-hypertension-treat-treat/ Photos: BP https://www.google.com/url?sa=i&url=https%3A%2F%2Fbloodpressureok.com%2Freading%2F190-over-115%2F&psig=AOvVaw0Vdzdftmt-_W2XDH-tYd3S&ust=1617841431472000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCMi20pLv6u8CFQAAAAAdAAAAABAD Finger laceration: https://www.google.com/url?sa=i&url=https%3A%2F%2Furgentmednetwork.com%2Fdoes-my-cut-require-urgent-care%2F&psig=AOvVaw1EI6ihTamhuZdc3d_wguBR&ust=1617841069415000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCLDspuft6u8CFQAAAAAdAAAAABAQ
- Photo credit: https://www.google.com/url?sa=i&url=https%3A%2F%2Fwww.slideshare.net%2Fdrvenugopalpp%2Fhypertensive-crisis-detection-and-management-in-ed&psig=AOvVaw1fw2nofP0lpgfZ3MLhY8RH&ust=1617839030906000&source=images&cd=vfe&ved=0CAMQjB1qFwoTCLixup_m6u8CFQAAAAAdAAAAABAP Elevated Asymptomatic Hypertension: To Treat or Not to Treat? https://rebelem.com/elevated-asymptomatic-hypertension-treat-treat/
- Photo: https://www.ahajournals.org/doi/10.1161/HYP.0000000000000065 *https://www.consultant360.com/articles/acute-hypertension-hypertensive-urgency-and-hypertensive-emergency#:~:text=Hypertensive%20urgency%20is%20defined%20as,anxiety%20but%20often%20are%20asymptomatic.
- High Blood Pressure and Hypertensive Crisis https://www.webmd.com/hypertension-high-blood-pressure/guide/hypertensive-crisis Hypertensive emergency https://wikem.org/wiki/Hypertensive_emergency
- Photo: https://www.paediatricfoam.com/2018/04/under-pressure-hypertensive-emergencies/ Photo: EOD https://encrypted-tbn0.gstatic.com/images?q=tbn:ANd9GcSjq6XVuHa4N1eTGV0v2m_iyGAS3iWwYYF2-Q&usqp=CAU https://emedicine.medscape.com/article/1952052-overview
- Malignant Hypertension https://emedicine.medscape.com/article/241640-overview
- Photo: http://www.emdocs.net/hypertensive-crisis-pearls-and-pitfalls-for-the-ed-physician/
- Image: https://www.semanticscholar.org/paper/Hypertensive-Emergency.-Suneja-Sanders/580a9435f7bcd6ba1dcc265b94d21a6af7ce0e65/figure/2
- https://emcrit.org/emcrit/hypertensive-emergencies/
- https://www.aafp.org/afp/2010/0215/p470.html Stroke care and BP photo and text: https://www.jems.com/patient-care/blood-pressure-management-goals-in-stroke-care/
- AAFP
- https://emedicine.medscape.com/article/1952052-overview#a2 Photo: http://www.emdocs.net/hypertensive-crisis-pearls-and-pitfalls-for-the-ed-physician/
- Internet Book of Critical Care (IBCC) https://emcrit.org/ibcc/hypertensive-emergency/#Algorithm_&_drug_tables
- https://emergencymedicinecases.com/episode-41-hypertensive-emergencies/ Medications and their use: https://wikem.org/wiki/Hypertensive_emergency
- Emergency Medicine Cases Episode 41: Hypertensive Emergencies https://emergencymedicinecases.com/episode-41-hypertensive-emergencies/ Photo: http://www.emdocs.net/hypertensive-crisis-pearls-and-pitfalls-for-the-ed-physician/ Hypertensive emergency is a medical emergency that requires prompt treatment with IV antihypertensives in attempts to reverse the ensuing multi-organ system failure. Calcium channel blockers and/or beta blockers remain the preferred treatment option for most cases of hypertensive emergency, with vasodilator serving as adjunctive agents when preload reduction is warranted. Although nicardipine is most commonly employed CCB, clevidipine has been increasingly in popularity due to its improved pharmacokinetics, ease of titratability, and lower risk of volume accumulation (max 1000mL/24hrs). Esmolol is ultra-short acting beta-1 selective blocker that is preferred for critically ill patients with organ dysfunction. In contrast labetalol is longer acting, and serves as a preferred agent for pregnancy-related hypertensive emergency or acute ischemic stroke. Labetalol should only be administered as an IV push for acute BP control NOT an IV infusion due to the risk of accumulation and prolonged toxicity. Nitroglycerin and nitroprusside are vasodilators that assist with preload reduction in states of congestion such as acute heart failure or pulmonary edema.
- https://emedicine.medscape.com/article/1952052-overview#a2 Photo: https://www.registerednursern.com/preeclampsia-eclampsia-nursing-maternity-review/
- Internet Book of Critical Care (IBCC) https://emcrit.org/ibcc/hypertensive-emergency/#Preamble:_Use_the_MAP MAP: https://www.google.com/url?sa=i&url=https%3A%2F%2Fwww.cvphysiology.com%2FBlood%2520Pressure%2FBP006&psig=AOvVaw2vu4hYoQG-Ng2nKiYzvSl3&ust=1617839506455000&source=images&cd=vfe&ved=0CAMQjB1qFwoTCMiFjf7n6u8CFQAAAAAdAAAAABAD MAP chart: https://www.google.com/url?sa=i&url=https%3A%2F%2Fwww.ahajournals.org%2Fdoi%2F10.1161%2FHYPERTENSIONAHA.120.14929&psig=AOvVaw2vu4hYoQG-Ng2nKiYzvSl3&ust=1617839506455000&source=images&cd=vfe&ved=0CAIQjRxqFwoTCMiFjf7n6u8CFQAAAAAdAAAAABAJ
- https://www.aafp.org/afp/2010/0215/p470.html https://www.acep.org/patient-care/clinical-policies/asymptomatic-elevated-blood-pressure/#sm.00000dnhqhmnuzf3guaxypz8x2i5z https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2527389 ACEP: Asymptomatic Elevated Blood Pressure (Feb 2013) https://www.acep.org/patient-care/clinical-policies/asymptomatic-elevated-blood-pressure/#sm.00000dnhqhmnuzf3guaxypz8x2i5z
- Case Resolution: https://rebelem.com/elevated-asymptomatic-hypertension-treat-treat/ Photo credit: https://post.healthline.com/wp-content/uploads/2019/10/Male_Hand_Wrap_732x549-thumbnail.jpg
- JNC 8 HTN Guideline Algorithm Jnc-8-hypertension-guideline-algorithm.pdf