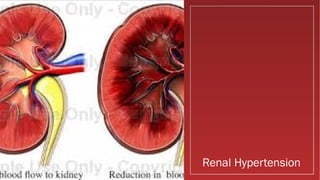
This document discusses hypertensive crises and hypertension. It defines normal blood pressure and stages of high blood pressure. Hypertensive crisis is a medical emergency occurring when blood pressure is above 180/110. The document outlines causes like lifestyle factors, risk factors like age and race, types of hypertension like malignant or renal, symptoms, complications affecting organs, diagnosis via blood pressure reading, emergency management using drugs to lower blood pressure, and long-term management.



















![Management In Emergency
• Fenoldopam, a peripheral dopamine-1-receptor agonist is given as
initial IV dose of 0.1 µg/kg/min titrated every 15 minutes.
• Clevidipine, a dihydropyridine calcium channel blocker, is
administered intravenously for rapid and precise BP reduction.[10]
It is
rapidly metabolized in the blood and tissues and does not accumulate
in the body.
As the BP approaches its goal, increase the clevidipine dose by less than
double, and lengthen the time between dose adjustments to every 5-
10 minutes. An approximately 1-2 mg/h increase produces an
additional 2-4 mm Hg decrease in SBP.](https://image.slidesharecdn.com/hypertensivecrisesranonshah-151220175025/85/Hypertensive-crisis-21-320.jpg)
























![Acute heart failure [MBBS]](https://cdn.slidesharecdn.com/ss_thumbnails/acuteheartfailure-170323061012-thumbnail.jpg?width=640&height=640&fit=bounds)
































































