Downloaded 16 times
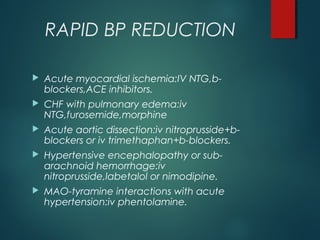
![DEFINITIONS
Systolic blood pressure >220 and diastolic >120mmHg.
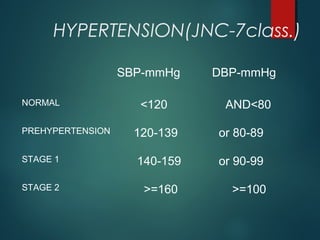
Patients with hypertension can be classified into 3 categories
based upon their symptoms and the organ systems that are
affected at the time of presentation:
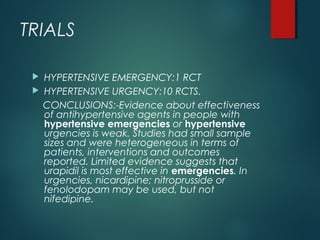
-HYPERTENSIVE EMERGENCY: also called hypertensive crisis, is severe
hypertension with acute impairment of an organ system (e.g.,
central nervous system [CNS], cardiovascular, renal). In these
conditions, the blood pressure (BP) should be lowered aggressively
over minutes to hours.Presence of papilledema indicates
MALIGNANT HYPERTENSION.
-HYPERTENSIVE URGENCY: the BP is a potential risk but has not yet
caused acute end-organ damage. These patients require BP
control over several days to weeks.
-ACCELERATED HYPERTENSION: recent significant increase over
baseline blood pressure that is associated with target organ
damage. This is usually vascular damage on fundoscopic
examination, such as flame-shaped hemorrhages or soft exudates,
but without papilledema.](https://image.slidesharecdn.com/sasihypertensiveemergensies-180326180318/85/Sasi-hypertensive-emergensies-8-320.jpg)



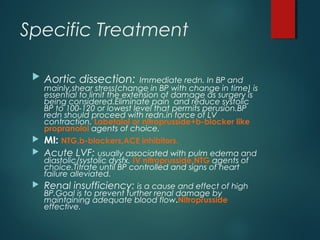
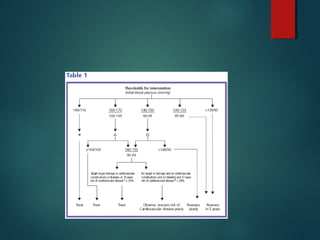

This document discusses hypertensive emergencies and urgencies. It defines hypertensive emergency as severe hypertension with acute end-organ damage, requiring rapid BP reduction over hours. Hypertensive urgency is severe hypertension without acute end-organ damage, allowing BP control over days to weeks. The main organs affected are the brain, heart, and kidneys. Initial treatment involves evaluating for end-organ damage and relaxing the patient before considering IV antihypertensives. Goals are to lower BP by 25% over the first hour while maintaining organ perfusion. Specific treatments depend on the damaged organ system. Follow-up after discharge assesses for ongoing hypertension management.













































![Hypertensive Crisis diagnosis treatment [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypertensivecrisis1-241128145637-9d731b1a-thumbnail.jpg?width=640&height=640&fit=bounds)





















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



