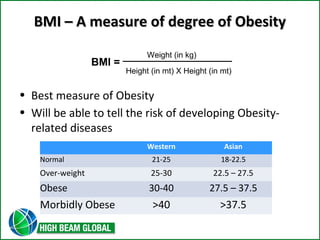
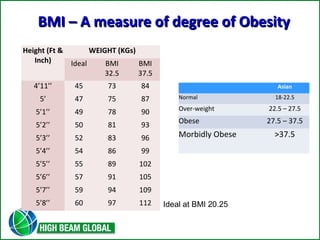
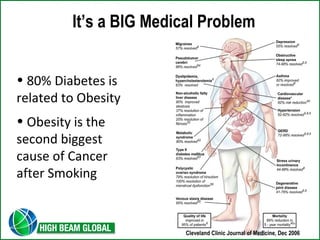
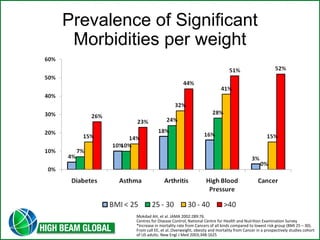
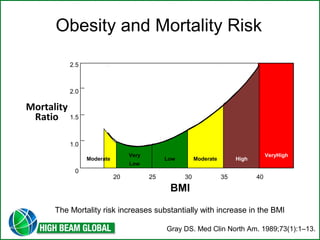
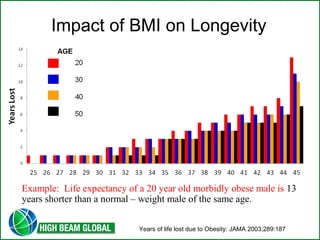
This document discusses total knee arthroplasty and surgical options for morbid obesity. It defines morbid obesity as having a BMI over 40 or over 37.5 for Asians. Surgical interventions like gastric bypass and sleeve gastrectomy are described as the most effective treatments for achieving significant and long-term weight loss for those with morbid obesity. These procedures work by restricting food intake and sometimes interfering with nutrient absorption. The risks of morbid obesity include diabetes, cancer, heart disease and early mortality which can be reduced through successful weight loss surgery.