Downloaded 139 times
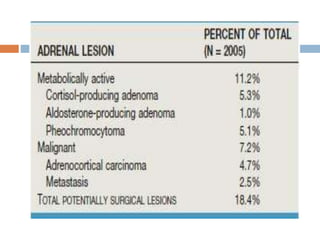








This document provides an overview of adrenal incidentalomas. It defines incidentalomas as unsuspected adrenal masses greater than 1 cm found on imaging for unrelated reasons. Nearly 20% may require surgery. Evaluation involves imaging to characterize the mass and metabolic testing to check for hormone hypersecretion. Computed tomography and MRI are used to identify lipid-rich adenomas. Biopsy has limited utility due to risk and inability to differentiate adenoma from carcinoma. Masses larger than 4 cm or those that grow over 1 cm may require resection. Metabolic testing evaluates for cortisol, catecholamine, aldosterone, and sex steroid hypersecretion, though sex hormone testing is not routinely recommended.

















































































