Downloaded 157 times
![Surgery Osce Quiz 2
http://jacknaimsnotes.blogspot.com/2010/02/surgery-osce-quiz-2.html
A 70 years old Malay man complaint of progressive abdominal pain for two weeks duration. the
pain is initially at the lower abdomen and then become generalized.
On examination, he was found to be dehydrated, febrile, ill-looking, generalized abdominal pain
with guarding and rebound tenderness at umbilicus.
He had undergone appendectomy 10 years ago.
After he was rehydrated, a laparotomy was performed to identify the problem and proceed
with necessary action. Below is the segment taken out from his stomach.
1) Identify the specimen
2) Outline your findings
3) What is your next management for this patient
For answer, click [here]](https://image.slidesharecdn.com/surgeryoscequiz2-100227120923-phpapp02/75/Surgery-Osce-Quiz-2-1-2048.jpg)
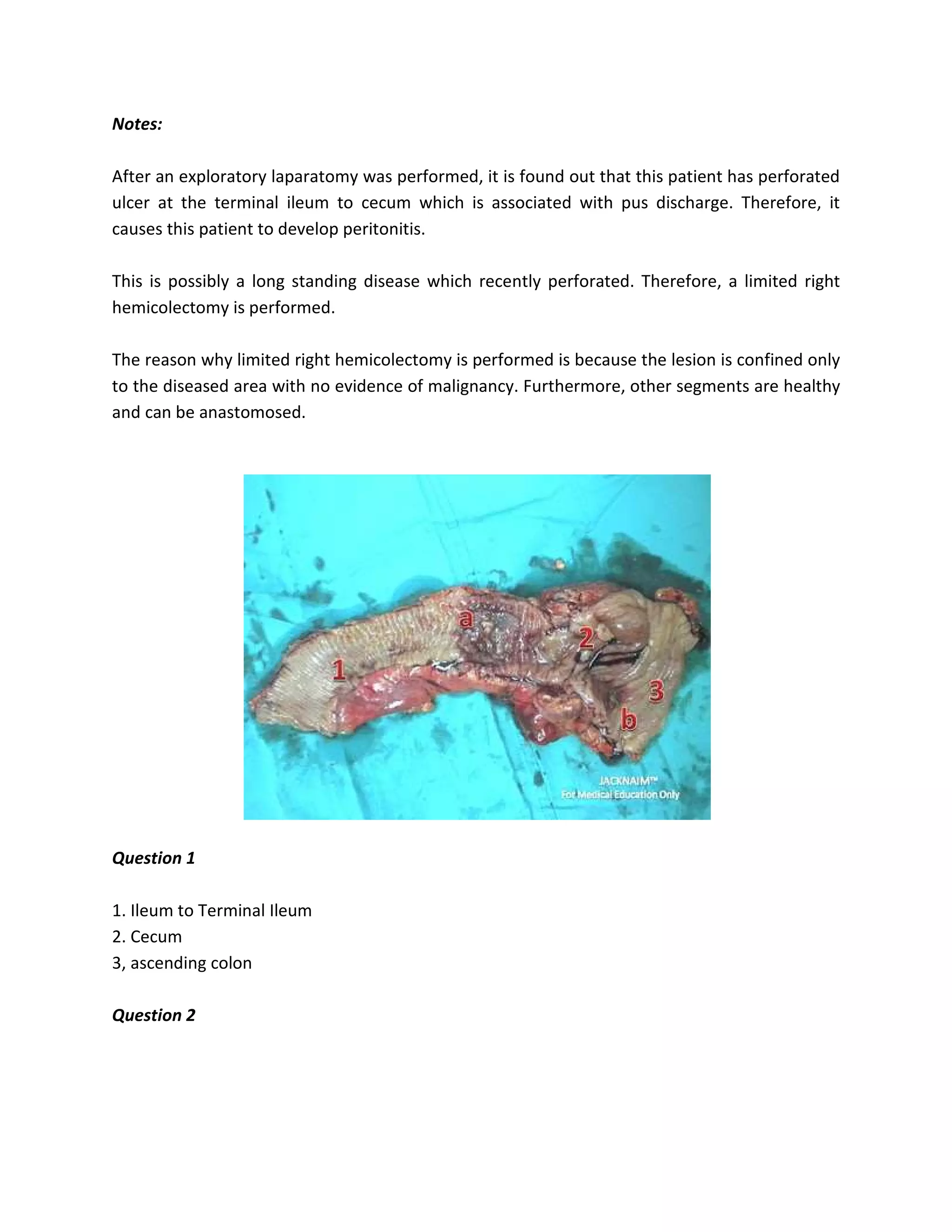


A 70-year-old man presented with progressive abdominal pain. On examination, he was found to be dehydrated, febrile, and had generalized abdominal pain with guarding and rebound tenderness. He underwent an appendectomy 10 years prior. After rehydration, an exploratory laparotomy revealed a perforated ulcer between the terminal ileum and cecum, causing peritonitis. A limited right hemicolectomy was performed to remove the diseased area. The patient's next steps included monitoring for complications, antibiotic treatment, and a post-operative diet.


































































































