Sudden onset shortness of breath in patient with chronic renal failure
•
3 likes•9,451 views


Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (17)
Similar to Sudden onset shortness of breath in patient with chronic renal failure
Similar to Sudden onset shortness of breath in patient with chronic renal failure (20)
More from AR Muhamad Na'im
More from AR Muhamad Na'im (20)
Recently uploaded
Recently uploaded (20)
Sudden onset shortness of breath in patient with chronic renal failure
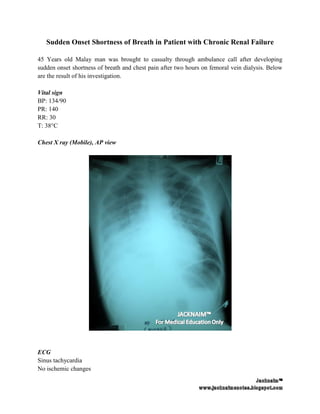
- 1. Sudden Onset Shortness of Breath in Patient with Chronic Renal Failure 45 Years old Malay man was brought to casualty through ambulance call after developing sudden onset shortness of breath and chest pain after two hours on femoral vein dialysis. Below are the result of his investigation. Vital sign BP: 134/90 PR: 140 RR: 30 T: 38°C Chest X ray (Mobile), AP view ECG Sinus tachycardia No ischemic changes
- 2. Renal Function Test Urea : 29.4 mmol/l Natrium : 131.7 mmol/l Pottasium : 5.2 mmol/l Chloride : 92.4 mmol/l Creatinine : 1389.9 µmol/l uric acid : 635 µmol/l CKMB : 20 U/l Full Blood Count WBC : 30.98 X103 (predominant neutrophil) HGB : 8.5 g/dL HCT : 28.8 Plt : 722 ABG under High flow mask 15L/min pH : 7.04 pCO2 : 35 mmHg pO2 : 66mmHg HCO3-: 9 mmol/L Questions 1) Outline the physiology function of kidney 2) Comment on the result of investigation 3) What is your provisional diagnosis 4) Outline your management to this patient.
- 3. Answer: 1) Physiology function of kidney a) Urine formation - Achieved by mechanism of glomerular filtration, tubular reabsorption and tubular secretion b) Elimination of body wastes and preservation of important metabolites and electrolytes. - Sodium and water re absorption - Regulation of sodium, chloride and potassium. - Glucose, amino acid and bicarbonate re absorption - Urea excretion which aid in concentrating the urine. -Ammonia secretion - Drug elimination from body. c) Regulation of blood pressure - Secretion of renin from juxtaglomerular cells to activate renin angiotensin aldosterone system(RAAS) in response to low sodium or low perfusion pressure. - Aldosterone increase sodium and water retention by collecting duct. - Depletion in inravascular volume will trigger release of vasopressin which act at collecting duct renal tubular apical plasma to increase free water absorpion by formation of water channels d) Regulation of calcium and phosphate metabolism - Hydroxylation of 25-hydroxycholecalciferol to enhance calcium absorption from gut. - Kidney is a site of action for PTH that increase calcium retention and phosphate secretion. e) Regulation of erythropoiesis - Kidney is the mainsite for erythropoietin secretion which is essential for stimulation of bone marrow production and red blood cell maturation. f) Production of Kinin - Kinin is a tissue hormones that act as vasodilator. It cause contraction of visceral smooth muscle but relax the vascular smooth muscle via Nitic oxide to lowered the blood pressure g) Regulation of acid based disorder - Achieved by regulation of hydrogen ion and bicarbonate.
- 4. 2) Comment on the result of investigation a) Chest X Ray - Presence of pleura effusion at right lung. - Peribronchial cuffing - increase blood flow to upper lobe • Finding consistent with pulmonary edema b) Renal function test - Elevation of urea, creatinine and uric acid which suggestive of renal impairment. c) Full blood count - Anemia of chonic illness - Markedly elevated white blood cell d) ABG - Non compensated severe metabolic acidosis - Low SPO2 concentration 3) Provisional diagnosis a) Acute pulmonary edema b) Sepsis (evidence of SIRS) with possible sources from femoral dialysis catheter. 4) Management of this patient Notes: most of the management has been done to this patient with result of investigation are attach above. However for the sake of discussion, full management is written here. a) Triage patient to the red zone b) Position the patient 90 degree (APO usually result in marked respiratory distress) c) Full monitoring of vital sign with cardiac monitoring. d) 100% Oxygen via high flow mask 15L/min. Consider the use of Non-Invasive Pressure Support Ventilation if available. e) Sublingual nitrates is the first line of treatment to decrease pulmonary vascular congestion. f) Watch out for impending respiratory failure which require patient to be intubated
- 5. - Altered mental status, poor and incoordinated respiratoy effort, progressive oxygen desaturation, ABG (PaO2 less than 50 mmHg or PaCO2 more than 50 mmHg. paC02 may be normal) [Shirley Ooi] g) Establish two large bore IV access h) 12 lead ECG to look for hyperkalaemic changes. i) Baseline ABG and blood investigation (FBC, Renal function test, cardiac enzyme) j) Portable Chest X Ray, AP view k) Bladder catherization to monitor urine output. l) IV morphine 0.1 mg/kg for pain management and to relieve the anxiety. (note that morphine is not initial choice for management of pulmonary edema eventhough it is a venodilator as it can further cause respiratory depression and lead to deterioration of patient condition) m) IV frusemide 40-80 mg Bolus. Since this APO are secondary to chronic renal failure, therefore larger dose may be needed. The dose may be repeated. n) Tip of femoral vein catheter for culture and sensitivity as well as blood culture. o) Starts patient on broad spectrum antibiotic. p) Treat the underlying acidosis with bicarbonate. q) Interventional dialysis 2-6 hours Discussion Chronic kidney injury is one of the major health problem in Malaysia with the top causes are due to hypertension, diabetic nephropathy, glomerulonephritis and lupus nephropathy. The only treatment for end stage renal failure are either life long dialysis or renal transplant. Dialysis even though very necessary in the treatment of chonic kidney disease because of fluid overload, hyperkalaemia, hyperuraemia and metabolic acidosis, it is related with many complication. Pulmonary edema is a pathological process in which the formation of fluid is more than the reflux in the lung interstitium; thereby more fluid is accumulated in the pulmonary interstitium and overflows into the alveoli [Shi Shen Wei et al, 2008] In early practical use of hemodylisis, the procedure itself is related to dialysis disequilibrium syndrome causing by the ‘urea reverse affect’. what happen is that, during dialysis, the rapid changes in the concentration of plasma urea and slow removal of urea from brain causing the formation of osmotic gradient between blood and brain. Hypertonic content of the brain attract water from blood vessel and causing the cerebral edema. This will resulting in neurological disturbance characterized by clinical symptoms like headache, muscular spasm, nausea, vomiting, brain swelling, seizure, coma, and even death
- 6. Another form of special type of DDS is the formation of acute respiratory distress syndrome which often being mistaken as acute pulmonary edema because of identical clinical feature. however the symptoms did not respind to treatment with cardiotonic drugs and the onset of disease is immediate after dialysis Pulmonary edema in chronic renal failure may be due to the delayed in scheduled dialysis, poor compliance to water/sodium restriction, inadequate fluid intake during last dialysis, deteriorating renal function with usual dialysis regimes is not working, and any insult resulting in formation of extra fluid in interstitial space In a study by using dog model to look for relationship between DDS with brain and lung pathology , Shi Shen Wei et al, found out that the pulmonary edema induced by hemodialysis can be excluded as caused by complement activation, acute pulmonary hypertension, neurogenic pulmonary edema, or water intoxication. The Radiologic Distinction of Cardiogenic and Noncardiogenic Edema, Milne et al, 1985
- 7. Reference: 1) Alfred Sacchetti, "Modern Management of Pulmonary Edema", Our Lady of Lourdes Medical Center 2) Eric N.C. Milne, Massimo Pistolesi, Massimo Miniati & Carlo Giuntini, "The Radiologic Distinction of Cardiogenic and Noncardiogenic Edema", AJR 144:879-894, May 1985. 3) Shirley Ooi & Peter Manning, Guide to the Essentials in Emergency Medicine, McGraw- Hill Education 4) Shi Zhen-wei and Wang Zhi-gang, "Acute cerebral and pulmonary edema induced by hemodialysis in a dog model", Chinese Medical Journal 2008; 121(11):1003-1009 5) Stephen J. McPhee, Vishwanath RL & William FG, "Pathophysiology of Disease: An Introduction to Clinical Medicine", 5th ed, Mc Graw Hill, 2006 6) William F. Ganong, "Review of Medical Physiology",21 ed, Mc Graw Hill, 2003