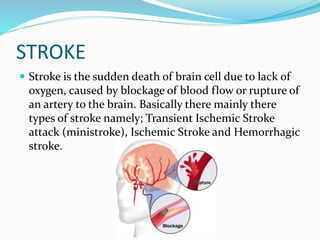
Strokes occur when blood flow to the brain is interrupted, either by a blockage or rupture of a blood vessel in the brain. There are three main types of strokes: transient ischemic attacks, ischemic strokes caused by blood clots, and hemorrhagic strokes caused by ruptured blood vessels. Signs of a stroke include muscular weakness, visual problems, speech difficulties, and headaches. Diagnostic tests include CT scans, MRI scans, and echocardiograms. Stroke treatment focuses on restoring blood flow, controlling risk factors, and rehabilitation to aid recovery.