Download to read offline























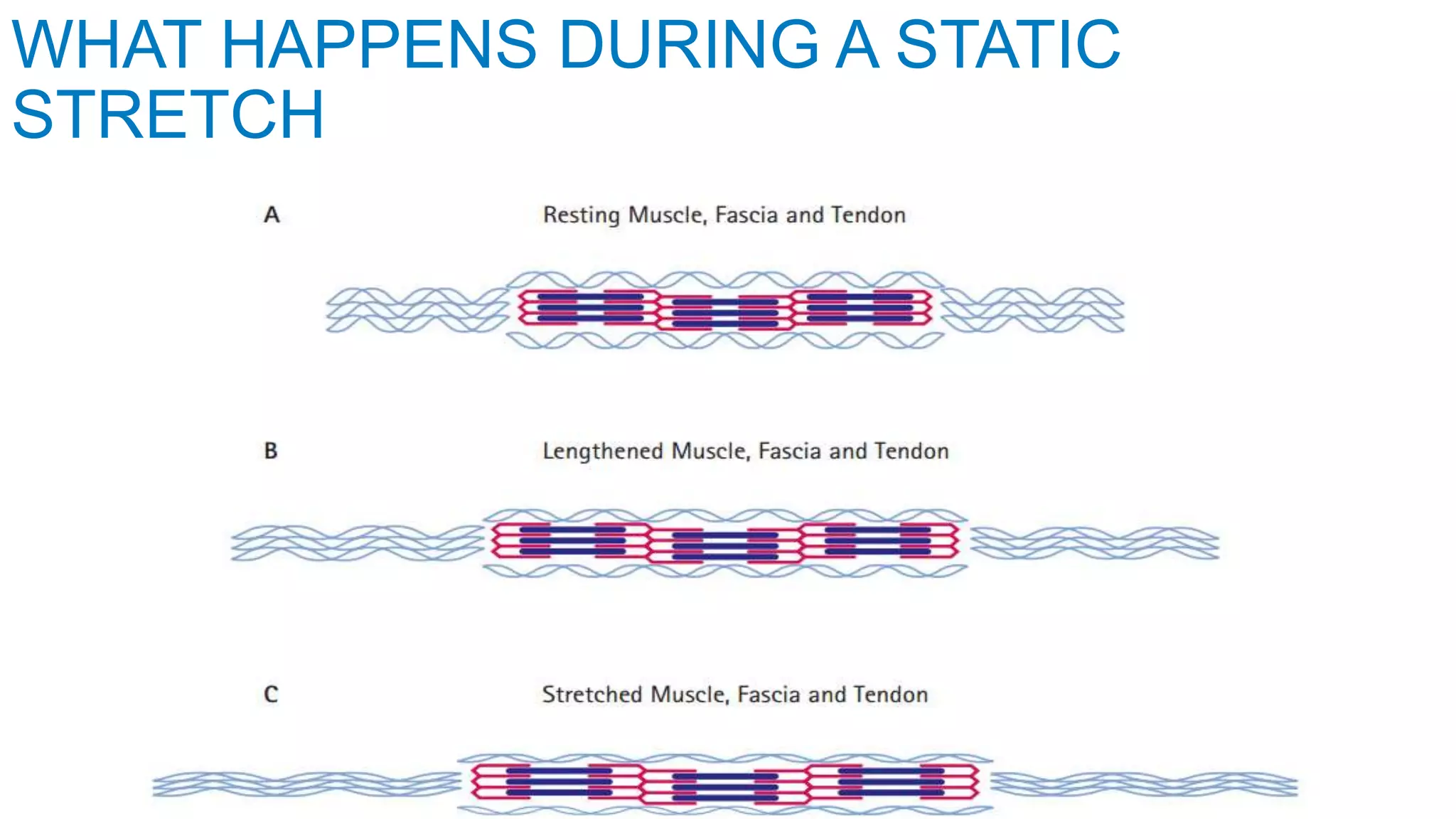











Stretching involves applying force to muscles and tendons to increase range of motion. It can improve flexibility and reduce injury risk. There are different types of stretching like static, dynamic, active, and passive. Flexibility is influenced by many factors and regular stretching provides benefits like increased mobility, reduced muscle soreness, lower back pain relief, and improved athletic performance. Proper form, duration, frequency, and intensity level should be used to safely gain flexibility over time in a progressive manner.












![J._CONTRAST_BATH_THERAPY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/j-230713132551-5c45004c-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



