Download as PDF, PPTX
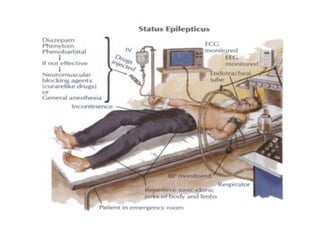
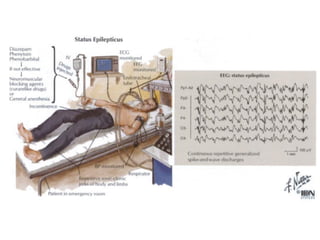



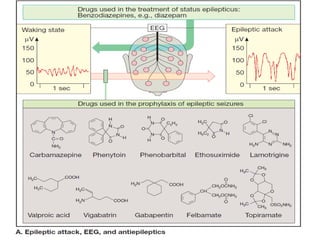
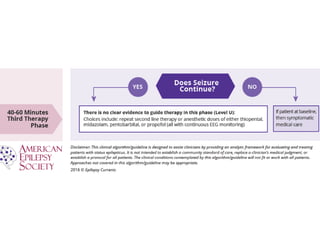

Status epilepticus is a life-threatening condition involving prolonged or repeated seizures without recovery between seizures. Intravenous administration of anti-seizure medications is required for treatment. Diazepam or lorazepam are usually effective for terminating seizures in the short-term, while phenytoin or fosphenytoin are preferred for prolonged therapy due to being highly effective with less sedation. If seizures are not controlled by first-line treatments, phenobarbital may be used, and refractory cases may require general anesthesia. Close monitoring is important due to risks of respiratory depression, hypotension, and cardiotoxicity from some medications.



















































































