Downloaded 69 times
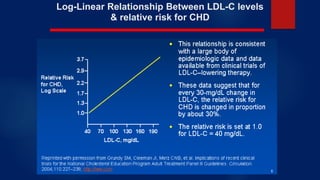
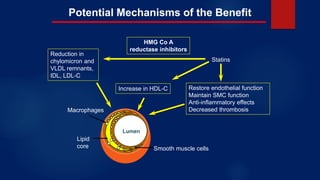
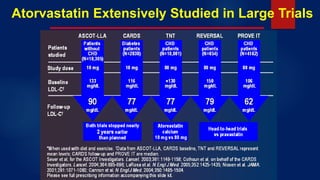
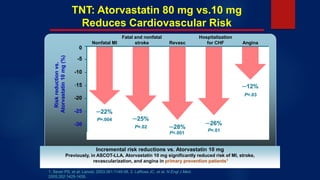
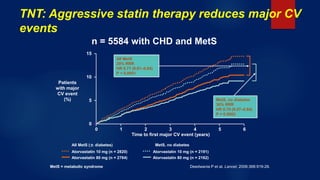
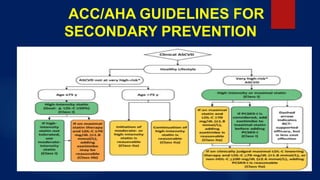
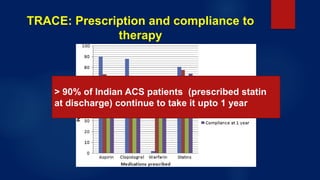


1) Statins are highly effective in reducing LDL-C and cardiovascular risk, playing a cornerstone role in lipid management. They work by inhibiting HMG-CoA reductase. 2) Atorvastatin has been extensively studied in large trials and shown to significantly reduce major cardiovascular events when doses are increased from 10 mg to 80 mg. 3) Studies in India found that high dose atorvastatin (80 mg) was well tolerated and more effective at reducing LDL-C and hs-CRP than lower doses in ACS patients. However, many ACS patients in India were not receiving statins as recommended.







































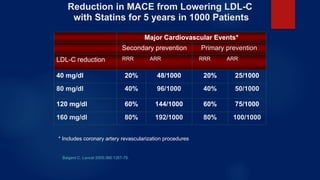
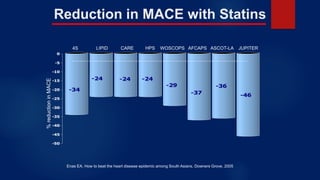
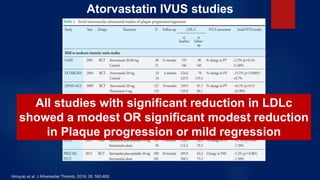
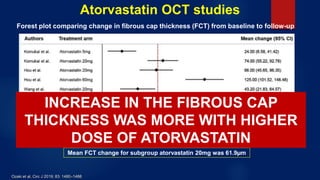
![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)















































