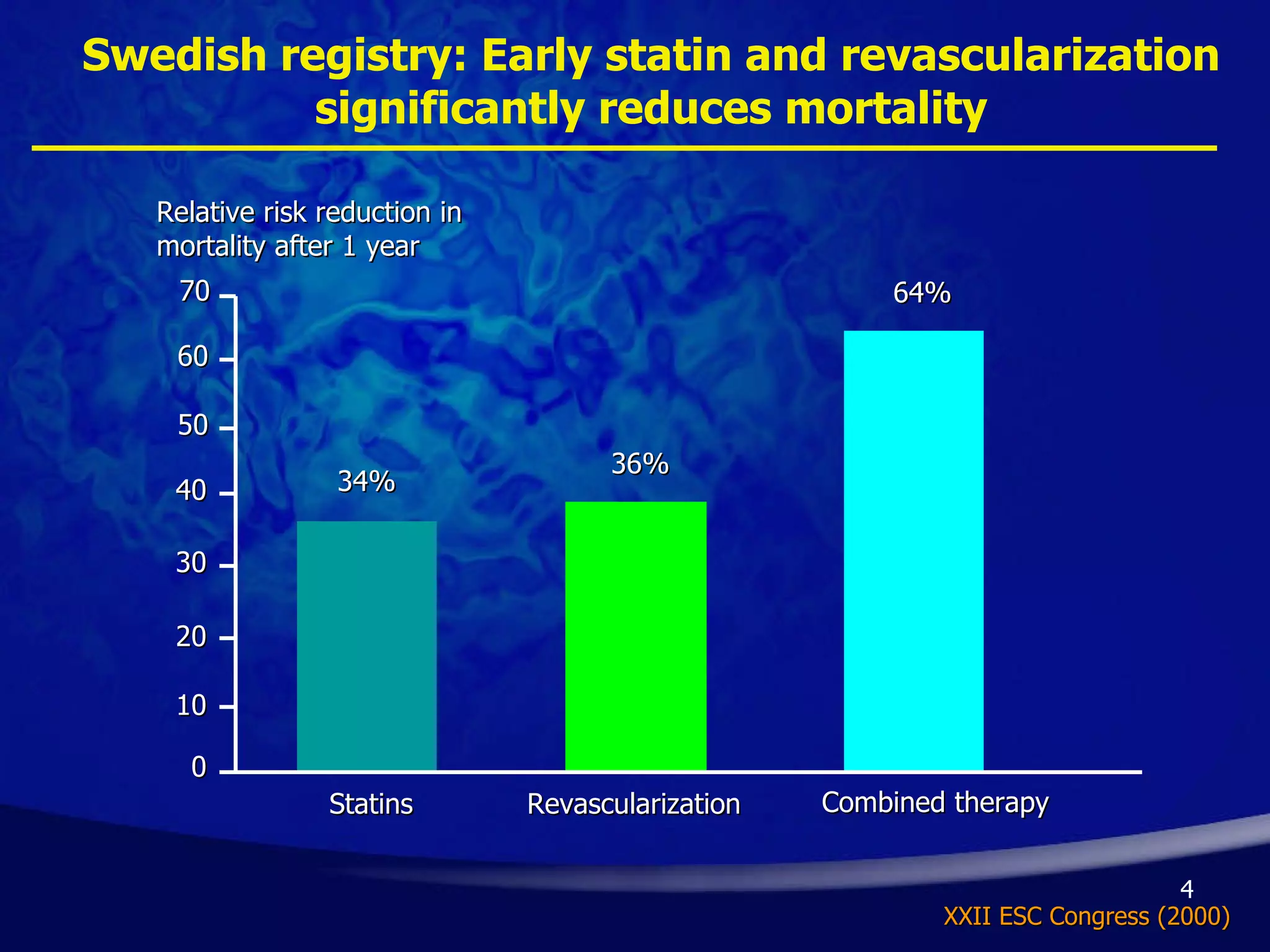
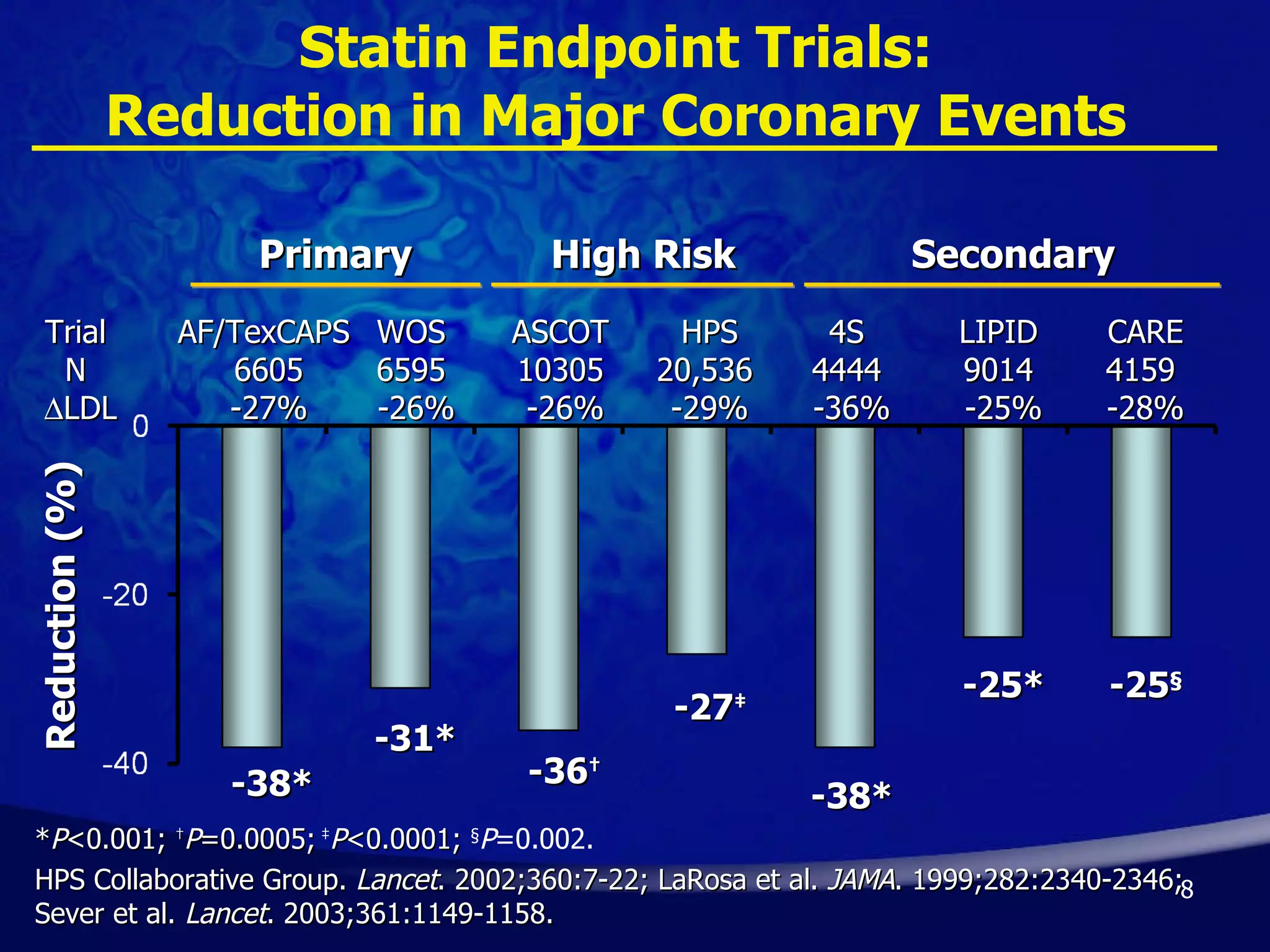
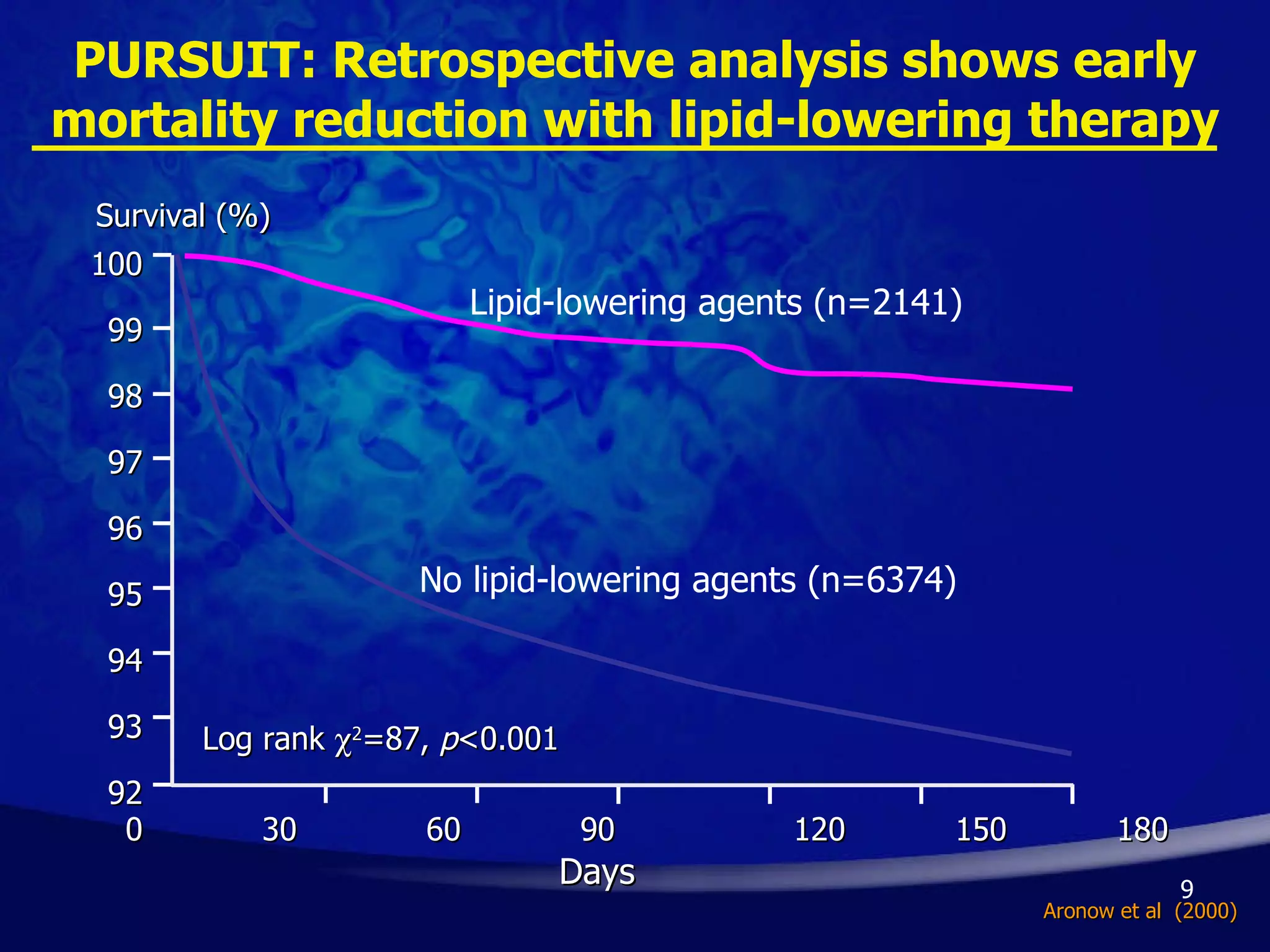
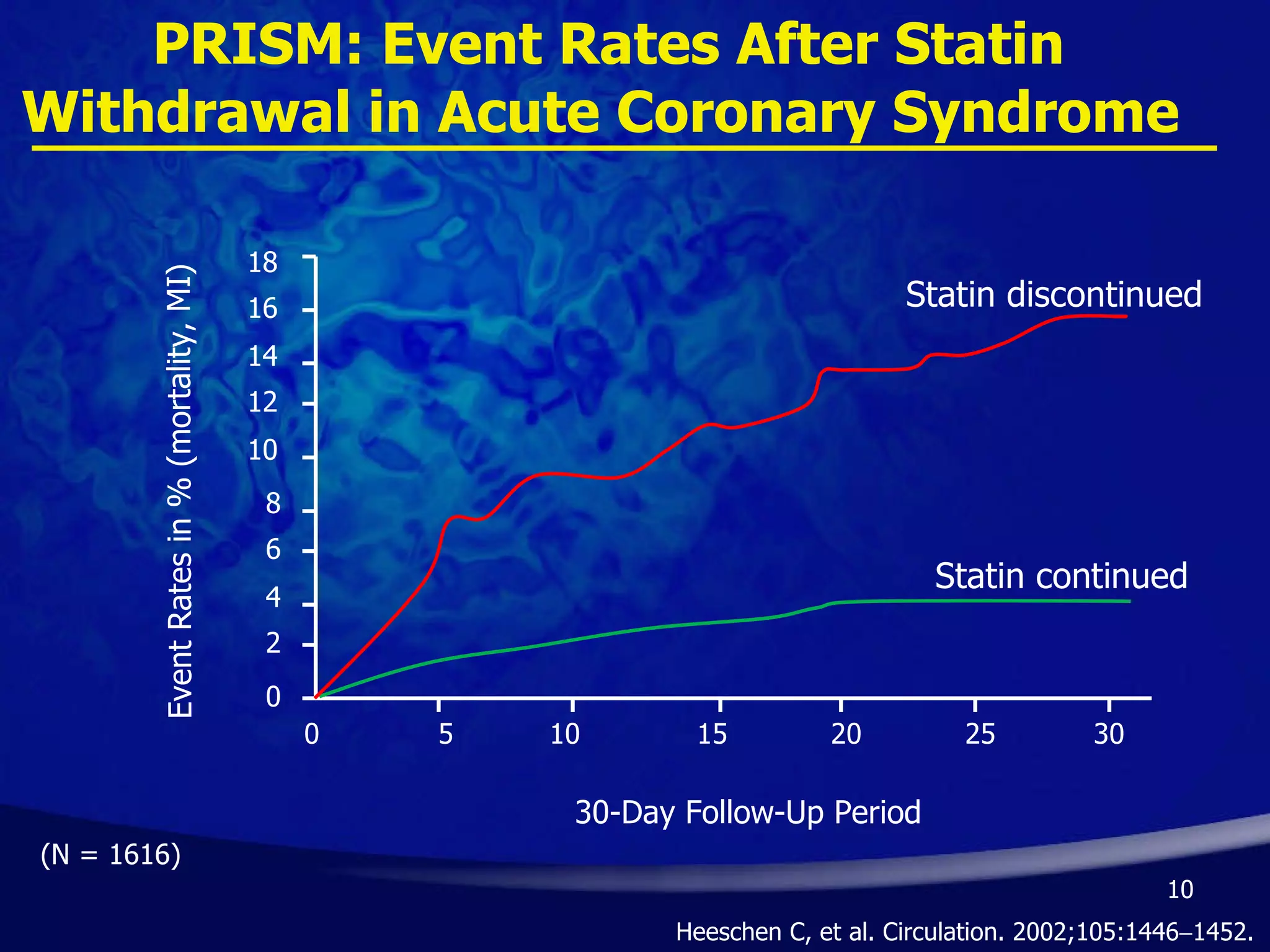
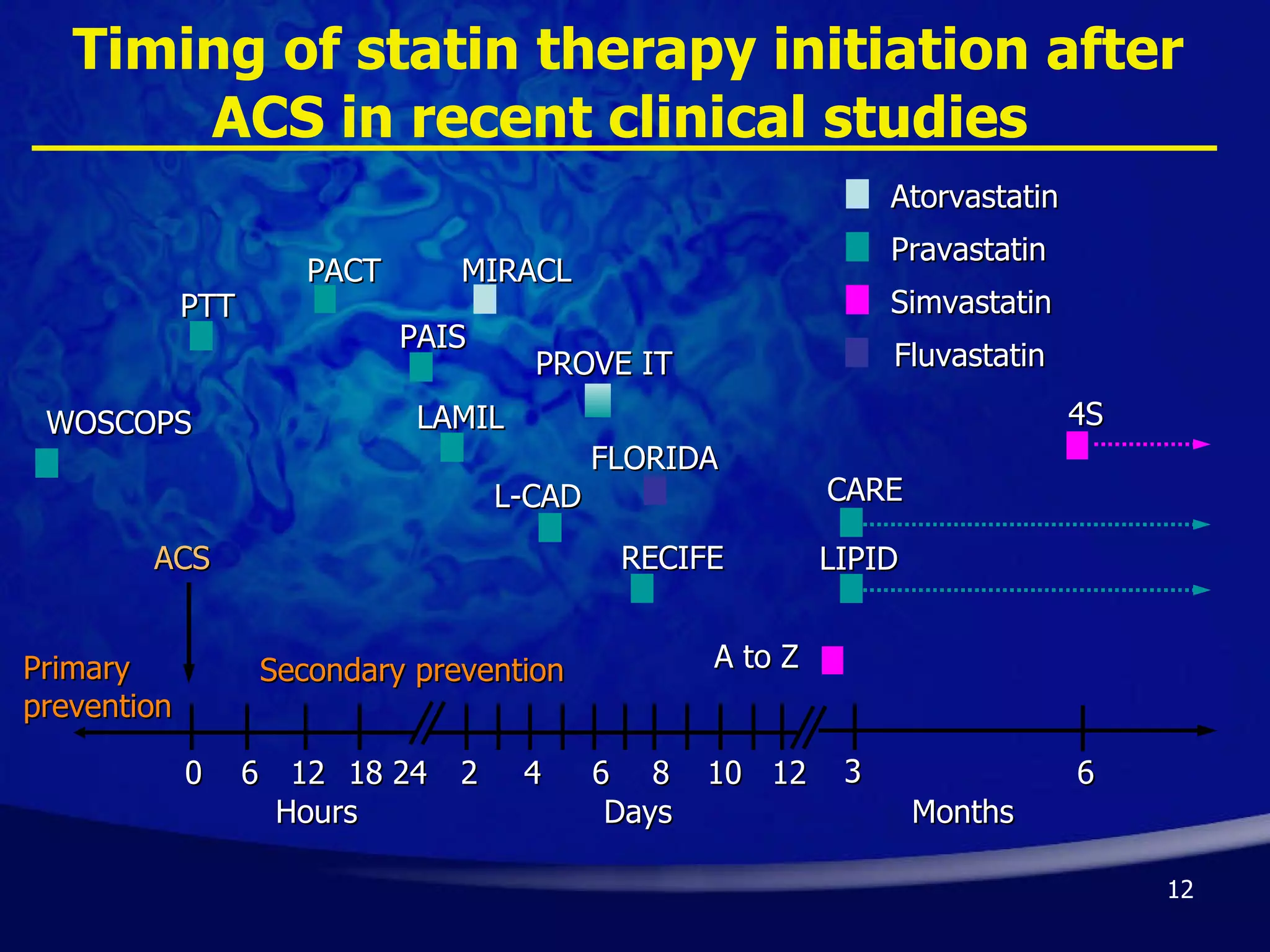
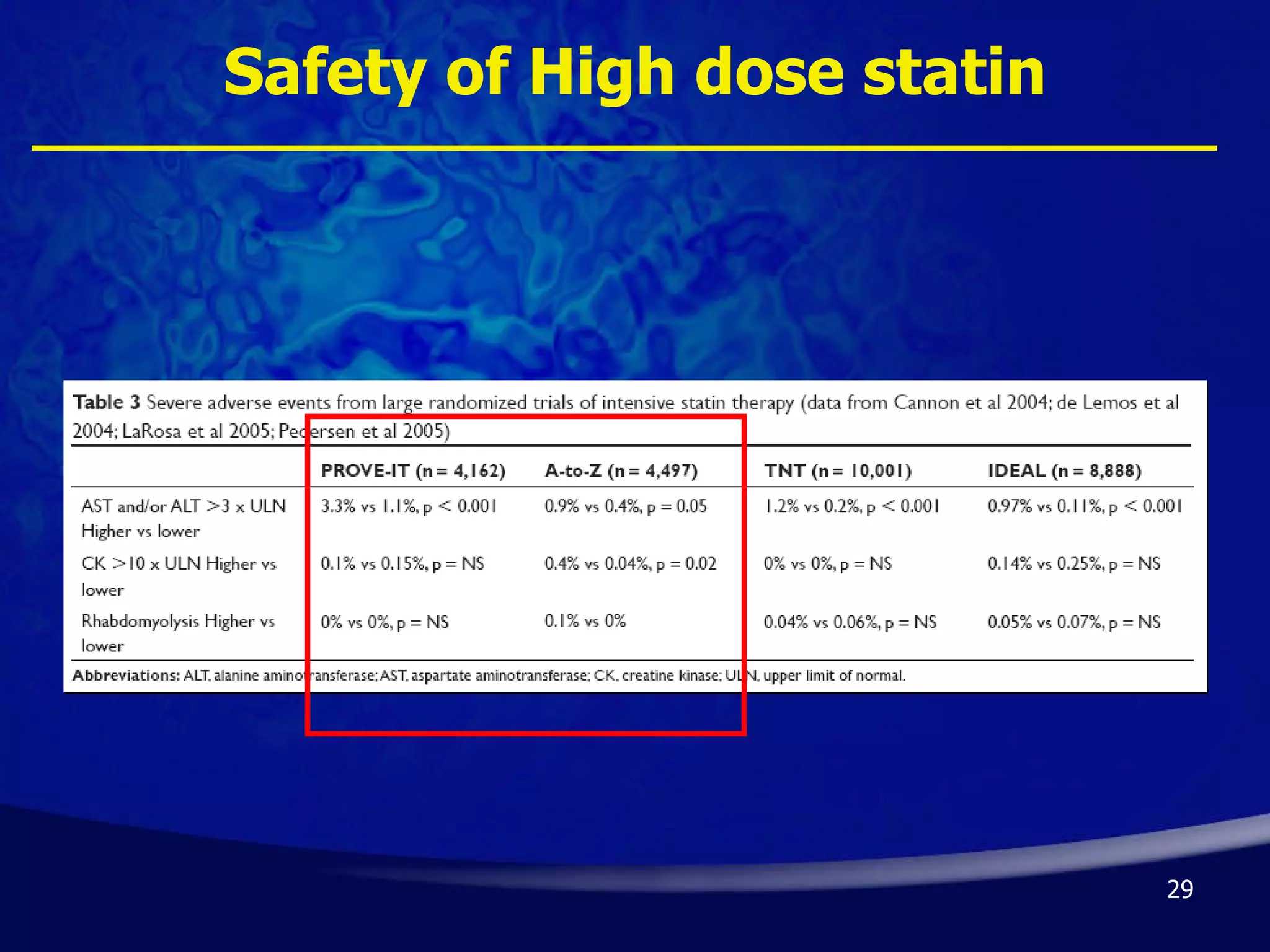
- Early initiation of high-intensity statin therapy in acute coronary syndrome patients significantly reduces mortality and morbidity rates compared to later initiation or lower-intensity statins. Clinical trials found a 16-36% reduction in major coronary events with early high-dose statin use.
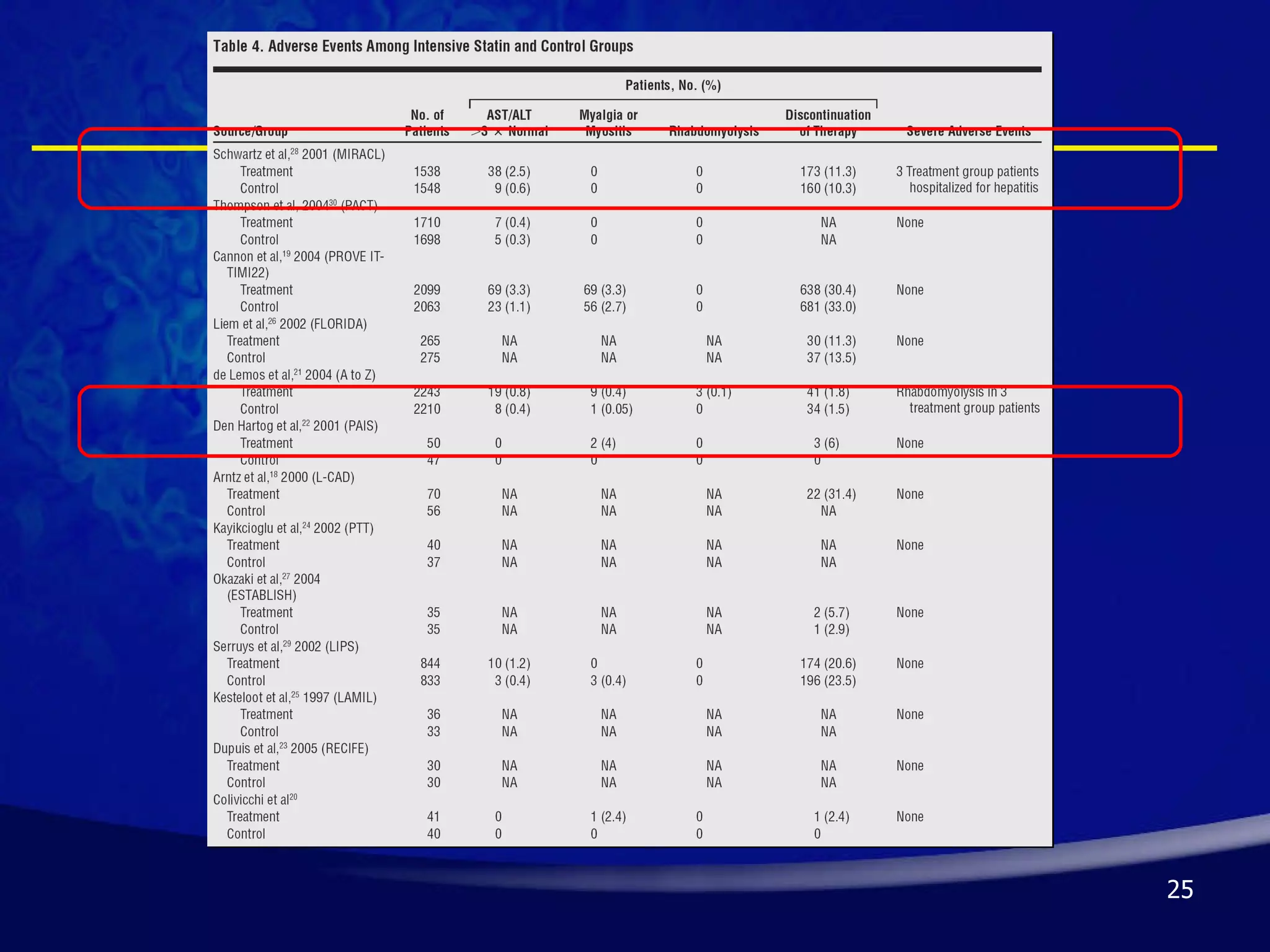
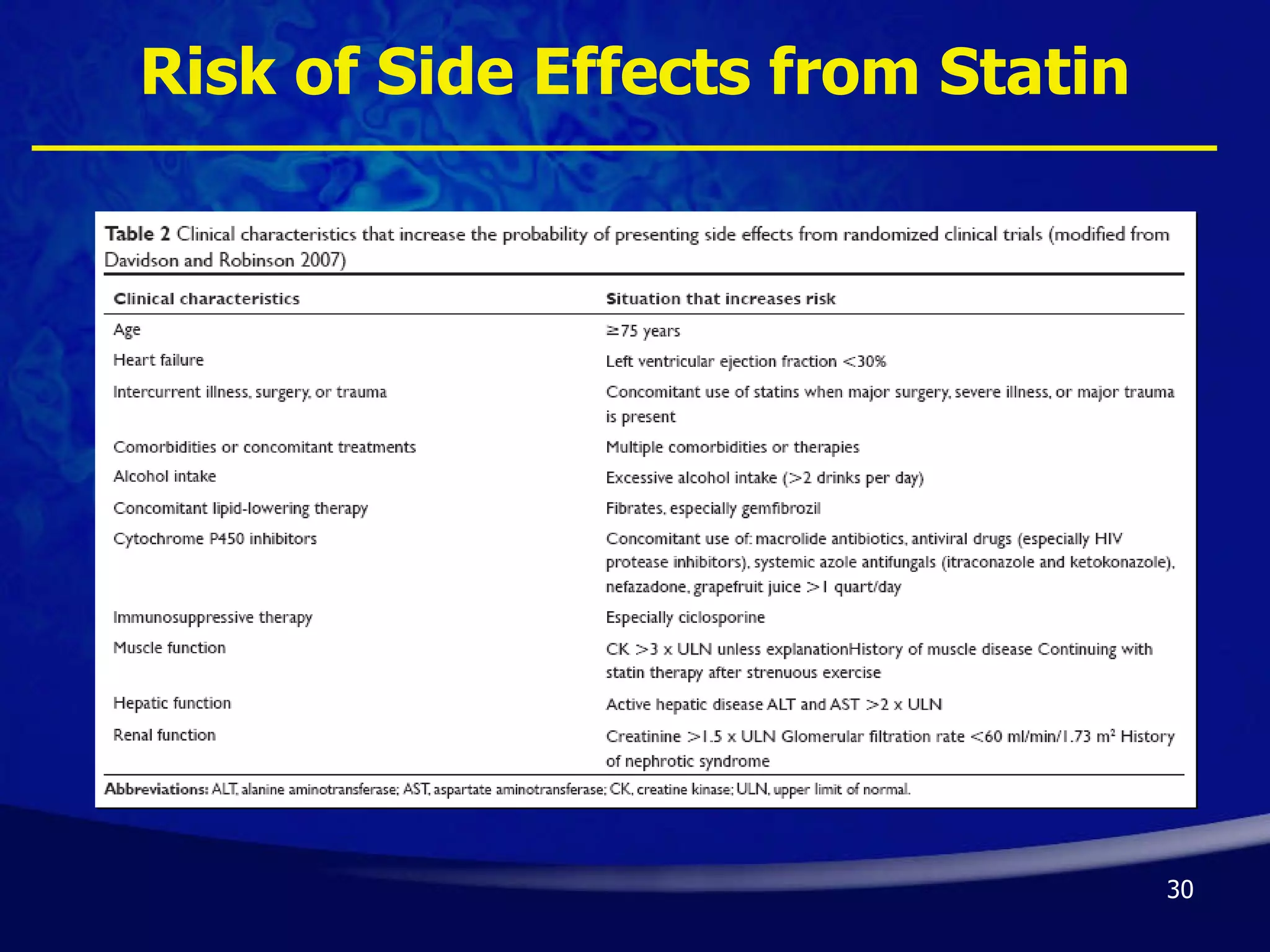
- Guidelines recommend high-intensity statins like atorvastatin 80mg or simvastatin 80mg for acute coronary syndrome patients, though risks like side effects must be considered. Long-term statin therapy is also generally advised after acute coronary syndrome.