Downloaded 15 times
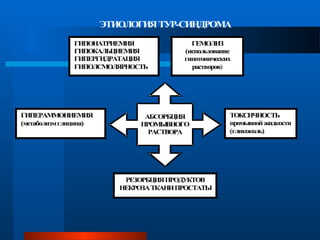
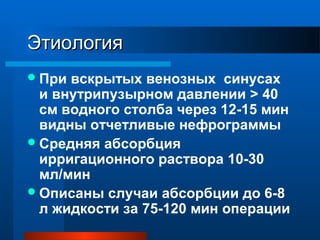
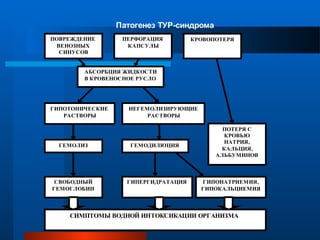
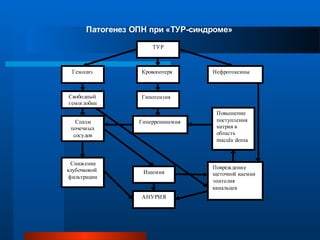

Тур-синдром, также известный как синдром водной интоксикации, возникает из-за резорбции значительных объемов промывочной жидкости во время трансуретральной резекции предстательной железы (ТУР). Этот синдром приводит к различным нарушениям гомеостаза, в том числе гипонатриемии и гипергидратации, с возможными тяжелыми осложнениями, такими как почечная недостаточность. Профилактика включает использование изоосмолярных растворов и мониторинг внутрипузырного давления во время операций.




































