This document defines and describes various aspects of human gait including:
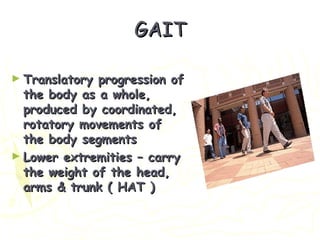
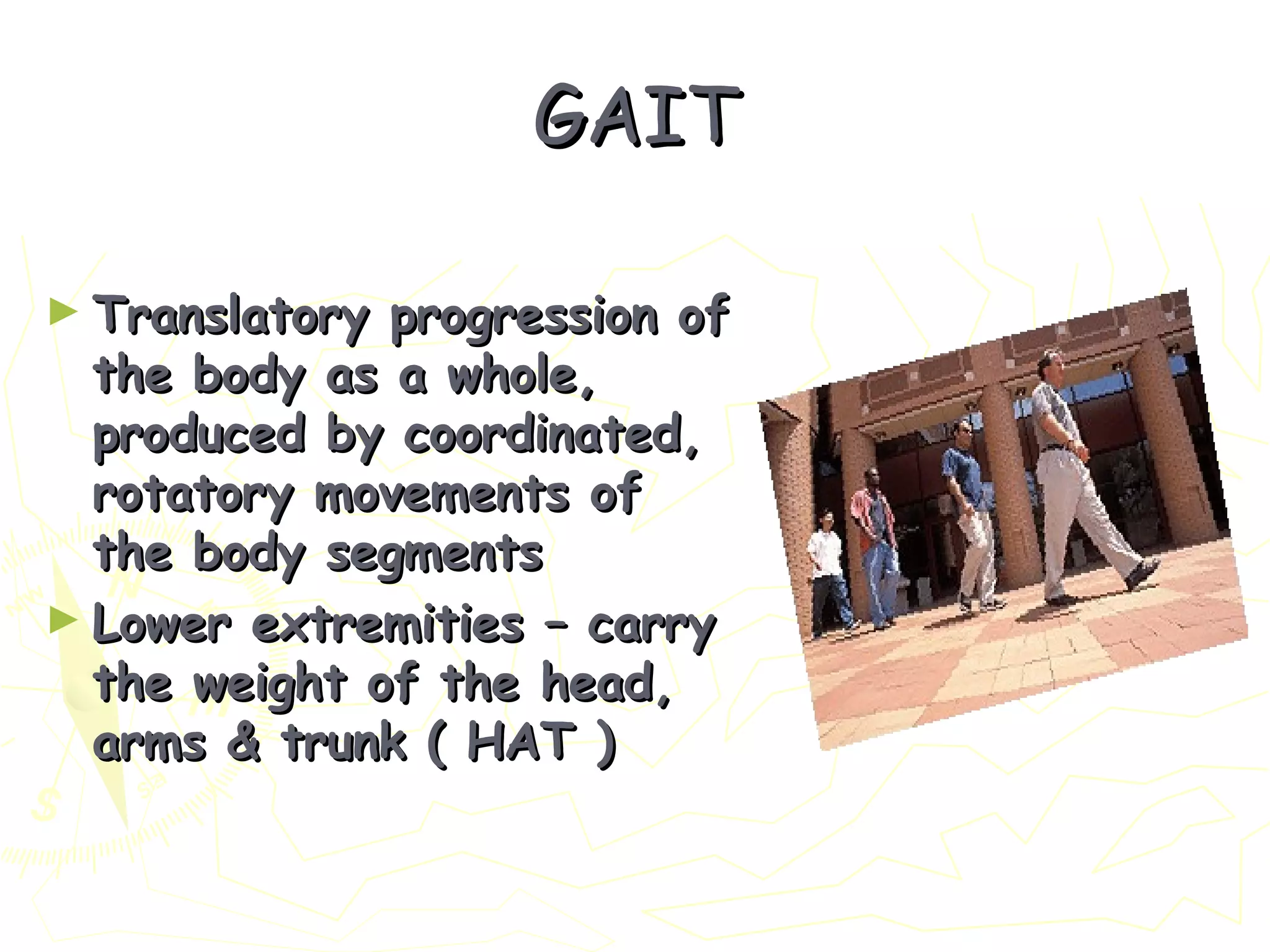
1. It provides definitions of gait from physiological, mechanical, and neurological perspectives. Gait involves coordinated movement of body segments to produce forward progression.
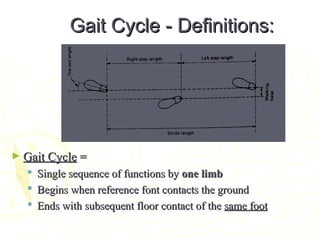
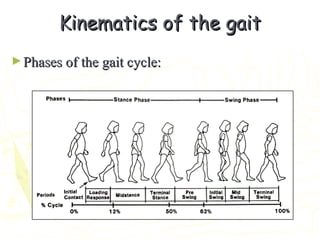
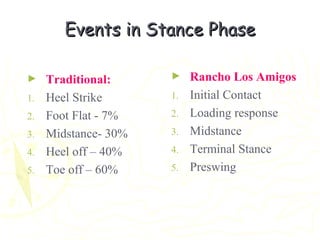
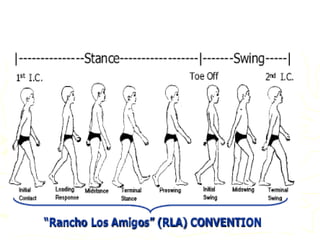
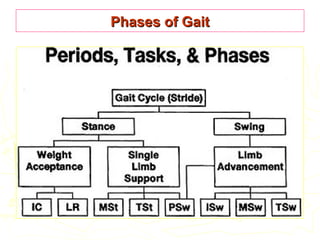
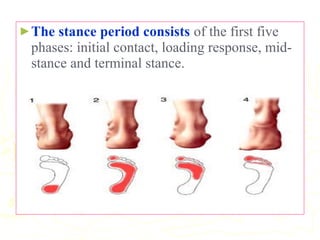
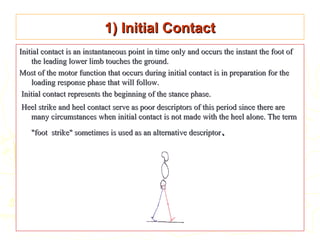
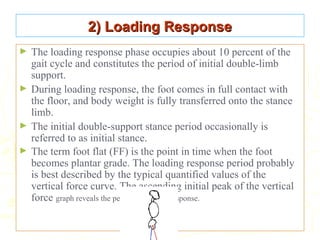
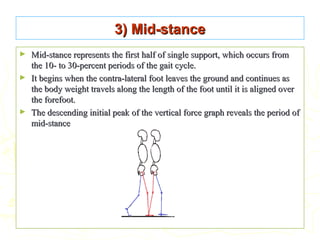
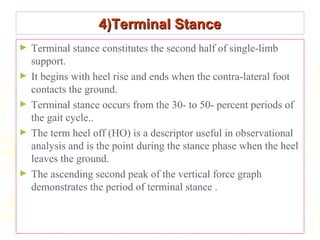
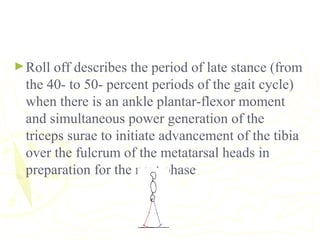
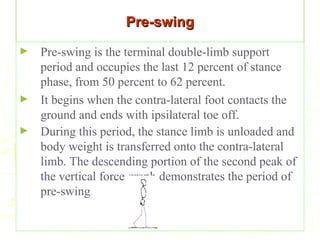
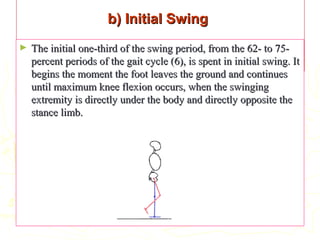
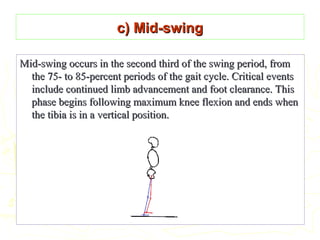
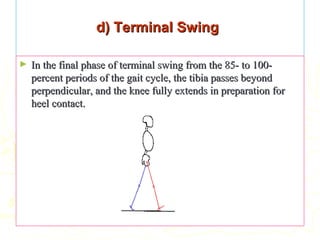
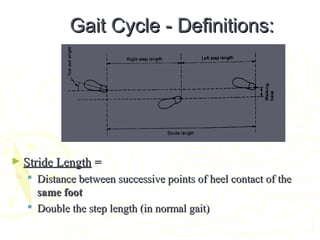
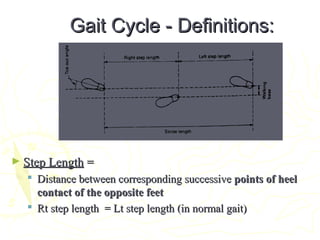
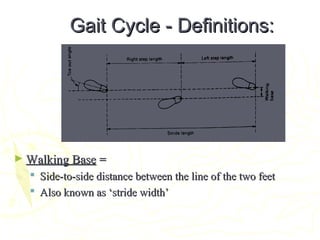
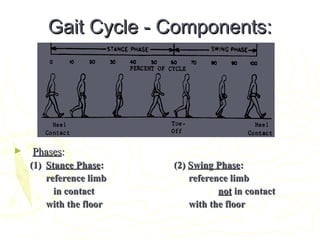
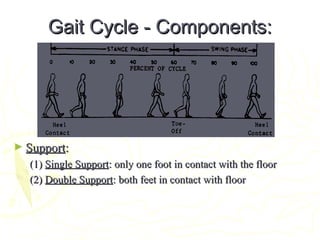
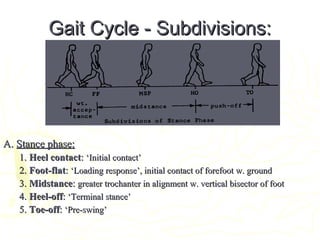
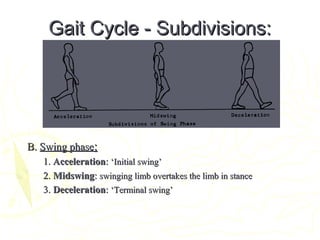
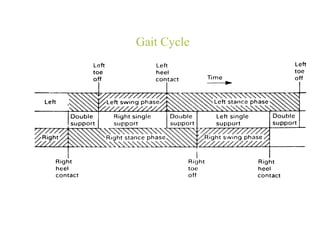
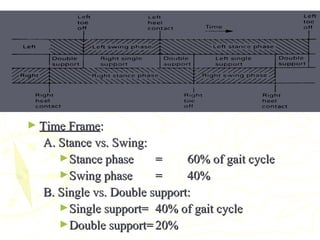
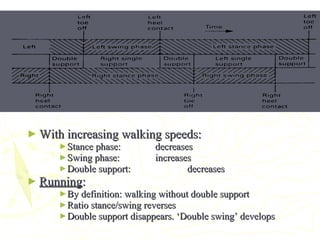
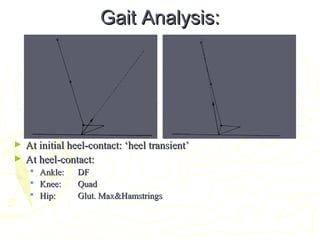
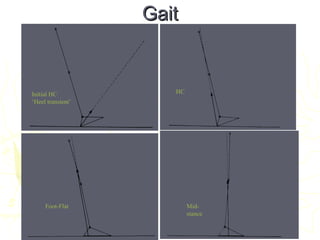
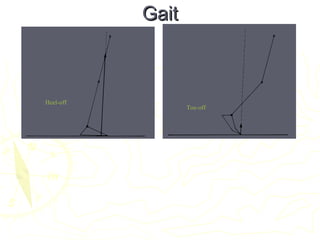
2. The gait cycle and its phases (stance, swing) are described in detail along with events within each phase like initial contact, loading response, mid-stance, terminal stance, pre-swing, initial swing, mid-swing and terminal swing.
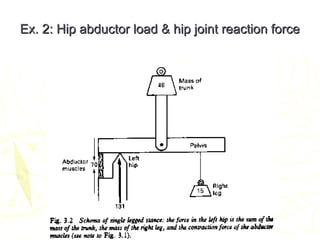
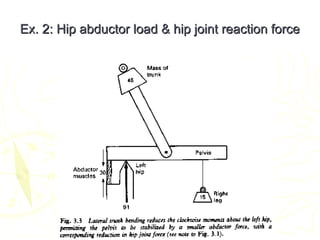
3. Prerequisites for walking including equilibrium, locomotion, musculoskeletal integrity and neurological control are outlined. Forces involved in gait production are also noted.
4. Purposes of gait like support, maintenance of


















































![GAIT and its different types[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gaitautosaved-240815185755-7939fafe-thumbnail.jpg?width=640&height=640&fit=bounds)























