Anatomy
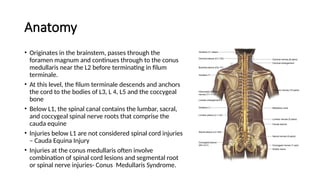
• Originates inthe brainstem, passes through the
foramen magnum and continues through to the conus
medullaris near the L2 before terminating in filum
terminale.
• At this level, the filum terminale descends and anchors
the cord to the bodies of L3, L 4, L5 and the coccygeal
bone
• Below L1, the spinal canal contains the lumbar, sacral,
and coccygeal spinal nerve roots that comprise the
cauda equine
• Injuries below L1 are not considered spinal cord injuries
– Cauda Equina Injury
• Injuries at the conus medullaris often involve
combination of spinal cord lesions and segmental root
or spinal nerve injuries- Conus Medullaris Syndrome.
3.
Anatomy cont…
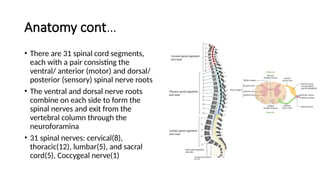
• Thereare 31 spinal cord segments,
each with a pair consisting the
ventral/ anterior (motor) and dorsal/
posterior (sensory) spinal nerve roots
• The ventral and dorsal nerve roots
combine on each side to form the
spinal nerves and exit from the
vertebral column through the
neuroforamina
• 31 spinal nerves: cervical(8),
thoracic(12), lumbar(5), and sacral
cord(5), Coccygeal nerve(1)
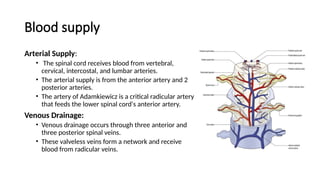
Blood supply
Arterial Supply:
•The spinal cord receives blood from vertebral,
cervical, intercostal, and lumbar arteries.
• The arterial supply is from the anterior artery and 2
posterior arteries.
• The artery of Adamkiewicz is a critical radicular artery
that feeds the lower spinal cord's anterior artery.
Venous Drainage:
• Venous drainage occurs through three anterior and
three posterior spinal veins.
• These valveless veins form a network and receive
blood from radicular veins.
6.
Spinal injury
Definition
• Aninsult to the spinal cord resulting in a change, either temporary or
permanent, in its normal motor, sensory, or autonomic function.
• Can be:
• Neural Tissue Injury
Spinal Cord Injury
Segmental Nerve injury
Combination Spinal Cord and Segmental Nerve Injury
Autonomic Nervous System Injury
• Vertebral Column Injury= Osteoligamentous Injury
7.
Epidemiology
• SCI ishighest among persons aged 16-30, in whom 53.1 percent of
injuries.
• Males represent 81.2 percent of all reported SCIs and 89.8 percent of all
sports-related SCIs.
• Among both genders, auto accidents, falls and gunshots are the three
leading causes of SCI.
• Sports and recreation-related SCI injuries primarily affect people under
the age of 29.
• Increased incidence among African Americans ( 27%) and Asians (2%)
• Most common causes are MVC (41%), falls, violence
9.
Pathophysiology
Primary spinal injuries:
•Direct physical trauma to vertebrae, ligaments, or the spinal cord
itself, causing compression, disruption, or blood supply disruption.
Secondary spinal injuries:
• Delayed biochemical changes that worsen initial neurological damage.
This includes decreased perfusion, edema and metabolic
accumulation.
10.
Types of spinalcord injury
Complete Spinal Cord Injury
• No sensory or voluntary motor function distal to the level of injury.
• Classified as ASIA A.
Incomplete Spinal Cord Injury
• Some neurologic function persists below the level of injury – the greater the
function distal to the injury the faster the recovery and the better the
prognosis
• Indicated by sacral sparing- perianal sensation, voluntary rectal motor
function, great toe flexor activity
11.
Complete spinal cordinjury
I. Tetraplegia(Quadriplegia): Spinal cord injury above the first thoracic
vertebra, or within the cervical sections of C1-C8. the result is some
degree of paralysis in all four limbs—the legs and arms.
II. Paraplegia: Spinal cord injuries below the first thoracic spinal levels
(T1-L5). Paraplegics are able to fully use their arms and hands, but the
degree to which their legs are disabled depends on the injury.
III. Complete paraplegia: It is described as permanent loss of motor and
nerve function at T1 level or below, resulting in loss of sensation and
movement in the legs, bowel, bladder, and sexual region.
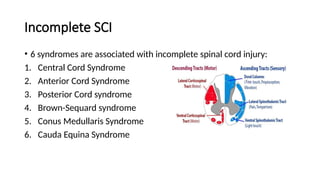
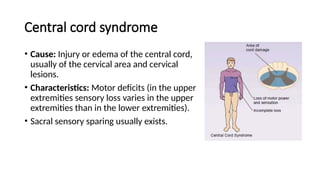
Central cord syndrome
•Cause: Injury or edema of the central cord,
usually of the cervical area and cervical
lesions.
• Characteristics: Motor deficits (in the upper
extremities sensory loss varies in the upper
extremities than in the lower extremities).
• Sacral sensory sparing usually exists.
14.
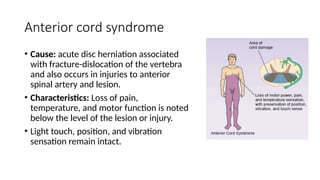
Anterior cord syndrome
•Cause: acute disc herniation associated
with fracture-dislocation of the vertebra
and also occurs in injuries to anterior
spinal artery and lesion.
• Characteristics: Loss of pain,
temperature, and motor function is noted
below the level of the lesion or injury.
• Light touch, position, and vibration
sensation remain intact.
15.
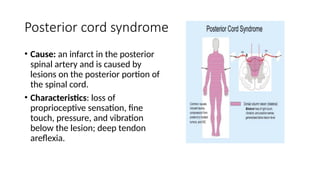
Posterior cord syndrome
•Cause: an infarct in the posterior
spinal artery and is caused by
lesions on the posterior portion of
the spinal cord.
• Characteristics: loss of
proprioceptive sensation, fine
touch, pressure, and vibration
below the lesion; deep tendon
areflexia.
16.
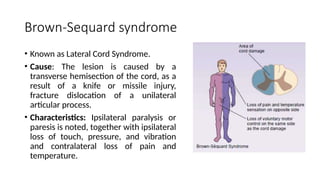
Brown-Sequard syndrome
• Knownas Lateral Cord Syndrome.
• Cause: The lesion is caused by a
transverse hemisection of the cord, as a
result of a knife or missile injury,
fracture dislocation of a unilateral
articular process.
• Characteristics: Ipsilateral paralysis or
paresis is noted, together with ipsilateral
loss of touch, pressure, and vibration
and contralateral loss of pain and
temperature.
17.
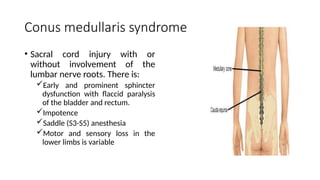
Conus medullaris syndrome
•Sacral cord injury with or
without involvement of the
lumbar nerve roots. There is:
Early and prominent sphincter
dysfunction with flaccid paralysis
of the bladder and rectum.
Impotence
Saddle (S3-S5) anesthesia
Motor and sensory loss in the
lower limbs is variable
18.
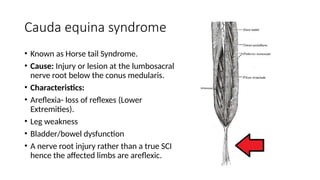
Cauda equina syndrome
•Known as Horse tail Syndrome.
• Cause: Injury or lesion at the lumbosacral
nerve root below the conus medularis.
• Characteristics:
• Areflexia- loss of reflexes (Lower
Extremities).
• Leg weakness
• Bladder/bowel dysfunction
• A nerve root injury rather than a true SCI
hence the affected limbs are areflexic.
19.
Types of shock
FeatureHypovolemic Shock Neurogenic Shock Spinal Shock
Cause Loss of blood volume
Disruption of sympathetic nervous
system pathways in the spinal cord
Physiological dysfunction following
spinal cord injury
Mechanism
Loss of blood volume leads to
decreased preload, which leads to
decreased cardiac output
Peripheral vasodilation, loss of
sympathetic cardiac innervation
Temporary loss of neural function
below injury level
Heart Rate Tachycardia (increased) Bradycardia (decreased) Variable (may be bradycardia initially)
Blood Pressure Hypotension (late stage)
Hypotension with low diastolic
pressure
Variable
Peripheral Perfusion Peripheral shutdown (cold, clammy) Warm, well-perfused areas Variable
Neurological Signs
None directly related to the nervous
system
Paralysis
Flaccid muscles, absent reflexes, loss
of sensation below injury level
Key Signs Tachycardia, Hypotension(late)
Bradycardia, Hypotension, Warm
extremities, Paralysis
Flaccid paralysis, absent reflexes,
absent bulbocavernosus reflex
Bulbocavernosus Reflex N/A N/A
Absent during spinal shock, present
after resolution
Duration Variable (depends on blood loss)
Variable (depends on spinal cord
injury)
Typically, less than 48 hours
20.
Spinal shock
• Astate of transient physiological (rather than anatomical) reflex
depression of cord function below the level of injury.
• Complete loss of all neurologic functions, including motor, sensory
and reflexes below the level of injury.
• End recognized by return of primitive reflexes caudal to the level of
injury usually 24 -48 hours Usually the bulbocarvenosus reflex or the
anal wink.
21.
Neurogenic shock
• Injuriesabove T6 disrupt the sympathetic nervous system to the heart
and the vascular system – Neurogenic shock
• Sympathetic disruption leads to encountered cholinergic action
leading to the triad of bradycardia,vasodilatation, hypotension
22.
Management of Spinalshock
• It involves maintaining hemodynamic and respiratory stability,
preventing further injury and providing supportive care.
• Patients with spinal shock may also have bradycardia hypotension i.e
neurogenic shock not due to causes other than the spinal cord injury.
• Patients with cervical and upper thoracic spinal cord injuries often
have respiratory depression, acute respiratory distress syndrome,
decreased cough reflex and poor secretion clearance.
• chest physiotherapy for respiratory management including
percussion, incentive spirometry and deep suctioning should be
employed.
23.
Management of neurogenicshock
• The most important treatment consideration is to maintain adequate
oxygenation and perfusion of the injured spinal cord.
• Judicious fluid replacement with isotonic crystalloid solution to a maximum of 2
liters is the initial treatment of choice.
• Overzealous crystalloid administration may cause pulmonary edema. To prevent
excessive fluid administration insert a pulmonary artery catheter.
• The therapeutic goal for neurogenic shock is adequate perfusion with:
SBP of 90-100 mmHg or a mean pressure of 70 mmHg
If fluid resuscitation is inadequate, to ensure organ perfusion, inotropic agents such as
dopamine 2.5 to 20.0 µg/kg per min and dobutamine 2.0 to 20.0 µg/kg per min may be
added to improve cardiac output and perfusion pressure.
Heart rate should be 60-100 beats per minute in normal sinus rhythm.
24.
Cont…
Hemodynamically significant bradycardiais treated with atropine 0.5
to 1.0 mg IV (every 5 min for a total dose of 3.0 mg).
Urine output should be more than 30 mL/h. Rarely, inotropic support
with dopamine is required in low urine output.
Ionotropic support with vasopressors may be required to maintain
blood pressures. Norepinephrine is recommended 1st
line.
Prevent hypothermia.
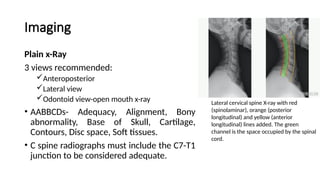
Imaging
Plain x-Ray
3 viewsrecommended:
Anteroposterior
Lateral view
Odontoid view-open mouth x-ray
• AABBCDs- Adequacy, Alignment, Bony
abnormality, Base of Skull, Cartilage,
Contours, Disc space, Soft tissues.
• C spine radiographs must include the C7-T1
junction to be considered adequate.
Lateral cervical spine X-ray with red
(spinolaminar), orange (posterior
longitudinal) and yellow (anterior
longitudinal) lines added. The green
channel is the space occupied by the spinal
cord.
28.
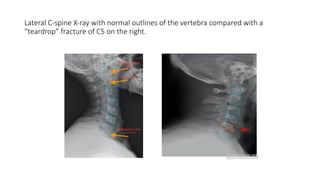
Lateral C-spine X-raywith normal outlines of the vertebra compared with a
“teardrop” fracture of C5 on the right.
29.
Imaging cont…
MRI
• Spinalcord injury – disruptions, oedema, haematomas
• Intervertebral disc disruption.
• Posterior ligamentous disruption.
• Canal compromise and neural tissue compression.
CT Scan
• CT scanning is reserved for delineating bony abnormalities or fractures.
• Assess occipitocervical and cervicothoracic junctions.
Cont…
Analgesics
• Start opioidanalgesia initially then NSAIDS
Bladder care: catheterization,
• Monitor the input-output of fluids initially.
• loss of bladder function
Bowel care
• Manual evacuation by sweeping through the rectum which causes irritation or the use of enemas(warm
soap enema)
NG tube
• Placement of a nasogastric tube for decompression.
• Ileus is common.
• This may also be used for nutritional support.
DVT prophylaxis.
• Use of medications or compression stockings.
33.
Cont…
• Anti emetics
•Aspiration pneumonitis is a serious complication in the SCI patient with
compromised respiratory function. Antiemetics should be used aggressively.
• Skin care
• Prevent pressure sores- Denervated skin is particularly prone to pressure necrosis.
• To prevent pressure sores:
• Remove the spine board as soon as possible.
• Undress the patient to remove belts and back pocket keys or wallets.
• Turn the patient every 1-2 hours.
• Nurse in Ripple Mattress or pneumatic mattresses,
• Pad all extensor surfaces.
• Apply Zinc Oxide cream
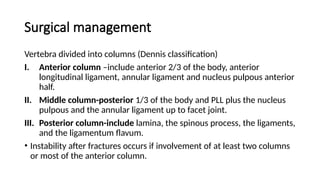
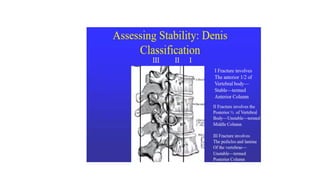
Surgical management
Vertebra dividedinto columns (Dennis classification)
I. Anterior column –include anterior 2/3 of the body, anterior
longitudinal ligament, annular ligament and nucleus pulpous anterior
half.
II. Middle column-posterior 1/3 of the body and PLL plus the nucleus
pulpous and the annular ligament up to facet joint.
III. Posterior column-include lamina, the spinous process, the ligaments,
and the ligamentum flavum.
• Instability after fractures occurs if involvement of at least two columns
or most of the anterior column.
37.
Cont…
Decompression
• Indicated ifa patient has an incomplete spinal cord injury and evidence of continued
neural element compression.
• Retropulsed bone can be removed or pushed back into place
Surgical stabilization
• For a burst fracture in which the posterior elements remain intact, treatment may
consist of an anterior vertebrectomy, strut grafting, and fusion without instrumentation.
• Brace the patient post-operatively without undue risk of graft displacement or spinal
instability.
• Use of rods and pedicle screws.
• Use of cages to stabilize burst fracture.
References
• Textbook, Baileyand love’s short practice of suregery, 25th
edition.
• textbook, Apley and Solomon’s system of orthopeidics and trauma-
injuries of the spine.
• https://www.slideshare.net/slideshow/spinal-cord-injury-sci-1661092
43/166109243
• Mescape: spinal cord injuries.
• Radiopedia.
• Uptodate: acute traumatic spinal cord injury.
PRE-HOSPITAL MANAGEMENT OFSPINAL
TRAUMA
• Early management of suspected injury to the spinal cord involves:
• Assessment and resuscitation according to ATLS protocol.
• Oxygen perfusion and prevention of secondary spinal cord injury.
• Management of life-threatening injuries.
• Immobilization with semi rigid cervical collars and sandbags.
• Log rolling and transport in a firm backboard.
• Early transfer to pressure care mattress to prevent pressure sores.
42.
PRIMARY SURVEY ANDMANAGEMENT OF
LIFE-THREATENING INJURIES
AIRWAY: Maxillofacial fractures, laryngeal injuries, Secretions, Fb
aspiration
• Look: cyanosis, use of accessory muscles of respiration, agitation/
depressed levels of consciousness, apnea
• Listen: noisy breathing, stridor, absent breath sounds, Hoarse voice
• Feel: air on the cheek or palm of your hand
• Management: Chin lift, Jaw thrust, Oropharynheal/ nasopharyngeal
airways
43.
Primary survey
Cervical spine:clues to spinal injury: flaccid anal sphincter, bradycardia and
hypotension, priapism,
Secondary survey: Loss of sensation, Quadriplegia, loss of reflexes,
tenderness along the cervical spine
• Rx: Restriction of movement using semi rigid cervical collar
Breathing:
• Look: Chest wall injuries, Assymetrical chest wall expansion, Cyanosis, use
of accessory muscle of respiration
• Listen: Noisy breathing, lack of breath sounds on auscultation, dullness or
hyperresonance on percussion
44.
• Feel: trachealdeviation
• Management: Decompression at the 2nd
ICS MC, Oxygenation using
BVM and NRM using 15-20l of oxygen, chest tube insertion
• Circulation: Active bleeding sites, fts of shock: tachycardia, tachypnea,
hypotension, altered CNS status, urine output,cool and clammy skin
• Rx: Torniquets, compression dressings, direct pressure, Tranexamic acid
1g IV accesss, Ringers lactate to a max of 2l
• Overzealous fluid resuscitation, pulmonary edema. Vasopressors
• Dobutamine 2-20 mcg/kg.min, dopamine 2.5-20mcg/kg/min. MAP: 70
45.
• Disability
• Environment:Prevent hypothermia using insulating blankets, warm
fluids
• Secondary survey for identification of injuries missed in primary
survey
• Here a neurological exam will identify sensory and motor deficits and
loss of reflexes which will be documented
46.
LOG ROLLING
• Techniqueused to move patients with suspected or confirmed spinal injuries
• PURPOSE: Maintain spinal alignment, prevent secondary spinal injury during
transport,
• Requires 4 assistants and good communication
• Manual in line stabilization of the neck and head, shoulder, hip and legs ,
patient is rolled away from the spinal board, spinal board is moved towards
the patient and patient is rolled onto the board
• Patient is then strapped at the forehead and shoulders, waist and legs
• https://youtu.be/Ewruf-w-0sA?si=WnOzWGjNkUekFqg1
• https://youtu.be/AlwFLh36kiE?si=7m4SiXf4EjNceBKC
47.
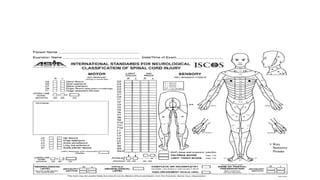
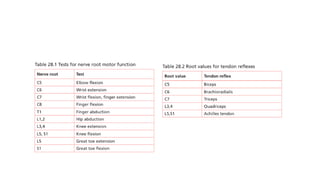
ASIA CHART
• Isa astandardized examination tool and reporting system for spinal cord
injuries:
• Components:
Patient, examiner name and date and time of exam
Motor components of the right and left upper and lower limbs with scores of 5 for
each myotome
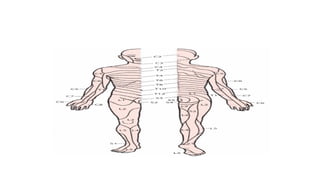
Sensory: 28 dermatomes with a max score of 2 where light touch and pain sensation
is assessed
Body maps for dermatome and myotome
Muscle grading
Interpretation: Neurological level, Incomplete/complete, ASIA iimpairment scale and
zones of partial impairment, clinical syndrome
51.
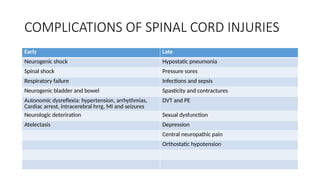
COMPLICATIONS OF SPINALCORD INJURIES
Early Late
Neurogenic shock Hypostatic pneumonia
Spinal shock Pressure sores
Respiratory failure Infections and sepsis
Neurogenic bladder and bowel Spasticity and contractures
Autonomic dysreflexia: hypertension, arrhythmias,
Cardiac arrest, intracerebral hrrg, MI and seizures
DVT and PE
Neurologic deteriration Sexual dysfunction
Atelectasis Depression
Central neuropathic pain
Orthostatic hypotension


















![Spinal cord injury [recovered]](https://cdn.slidesharecdn.com/ss_thumbnails/spinalcordinjuryrecovered-201022180848-thumbnail.jpg?width=640&height=640&fit=bounds)




















































