INTRODUCTION
• Cesarean section(CS) is the most commonly performed major
surgical procedure worldwide.
• Initially, general anesthesia (GA) was primarily used, leading to
high maternal mortality.
Anesthesia-related maternal mortality has reduced significantly
due to-Increased use of neuraxial anesthesia for CS.
Availability of algorithms and airway devices for performing
general anesthesia.
• Maternal mortality following general anesthesia was the
primary motivator for the transition toward greater use of
neuraxial anesthesia, for CS
3.
CAESAREAN SECTION
“It isdefined as the birth of an infant through incision
in the abdomen(laparotomy) and
uterus(hysterotomy).”
(derived from the latin word caedere which imply to cut)
4.
INDICATIONS FOR CAESAREANSECTION
Absolute
Absolute
Maternal
Cephalo-pelvic Disproportion
Non progression of labour
Fetal:
Fetal Distress
Non-cephalic presentations
Multiple gestations
Pregnancy Related
Abruptio Placenta
Grade 3 or 4 Placenta Praevia
Cervical obstructive lesions
Large vulvar condylomata
Relative
Relative
Maternal
Relative CPD
Maternal preference
Fetal:
Twins with first in non
cephalic presentation
Pregnancy Related
Lesser degrees APH
Previous Caesarean
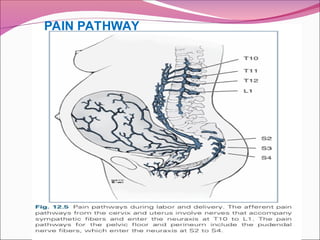
PAIN PATHWAYS
During CaesareanSection:
Pain due to Incision – Pfannensteil / Midline
Pain due to stretching to the skin and
subcutaneous tissues
Intraperitoneal dissection and manipulation
Additional somatic pain due to diaphragmatic
stimulation
Involves dermatomes up to T8 and visceral pain
pathways up to T4 levels
Implications: Aim is to achieve T4 dermatomal
level
ANAESTHESIA FOR CESAREANSECTION
Techniques of Anaesthesia:
1. Regional Anaesthesia
• Subarachnoid Block(Spinal)
• Epidural Anaesthesia
• Combined Spinal-Epidural Anaesthesia
2. General anaesthesia
3. Local anaesthesia
9.
Anaesthesia for CesareanSection…..
Depends on:
• Indication for CS
• Urgency of the procedure
• Maternal and fetal health
• Maternal desires
If time not a factor RA preferred
Epidural for Labour Analgesia in-situ Extension
of Block
RA contraindicated, or Emergency procedure
GA
10.
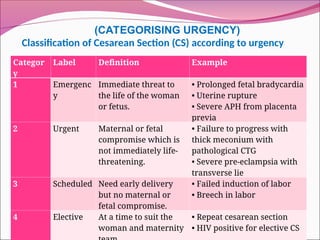
Classification of CesareanSection (CS) according to urgency
Categor
y
Label Definition Example
1 Emergenc
y
Immediate threat to
the life of the woman
or fetus.
• Prolonged fetal bradycardia
• Uterine rupture
• Severe APH from placenta
previa
2 Urgent Maternal or fetal
compromise which is
not immediately life-
threatening.
• Failure to progress with
thick meconium with
pathological CTG
• Severe pre-eclampsia with
transverse lie
3 Scheduled Need early delivery
but no maternal or
fetal compromise.
• Failed induction of labor
• Breech in labor
4 Elective At a time to suit the
woman and maternity
• Repeat cesarean section
• HIV positive for elective CS
(CATEGORISING URGENCY)
11.
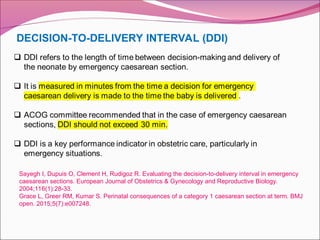
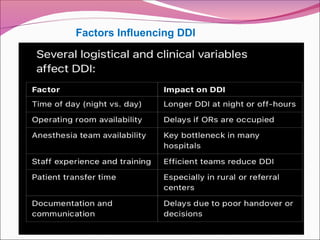
DECISION-TO-DELIVERY INTERVAL (DDI)
SayeghI, Dupuis O, Clement H, Rudigoz R. Evaluating the decision-to-delivery interval in emergency
caesarean sections. European Journal of Obstetrics & Gynecology and Reproductive Biology.
2004;116(1):28-33.
Grace L, Greer RM, Kumar S. Perinatal consequences of a category 1 caesarean section at term. BMJ
open. 2015;5(7):e007248.
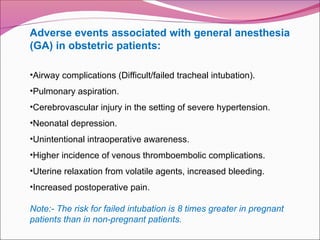
Adverse events associatedwith general anesthesia
(GA) in obstetric patients:
•Airway complications (Difficult/failed tracheal intubation).
•Pulmonary aspiration.
•Cerebrovascular injury in the setting of severe hypertension.
•Neonatal depression.
•Unintentional intraoperative awareness.
•Higher incidence of venous thromboembolic complications.
•Uterine relaxation from volatile agents, increased bleeding.
•Increased postoperative pain.
Note:- The risk for failed intubation is 8 times greater in pregnant
patients than in non-pregnant patients.
17.
REGIONAL ANAESTHESIA
Definitive benefitsover GA, including
No risk of aspiration
No risk of failed intubation or ventilation
Less blood loss
Less fetal exposure to drugs
Better neurobehavioral score of fetus at birth
Analgesia can be extended to postoperative period
Early skin to skin contact of neonate with
mother(better mother baby bonding)
Simple and inexpensive procedure.
18.
Contraindications to neuraxialanesthesia for cesarean
section:
• Patient refusal or inability to cooperate.
•Increased ICP secondary to a mass lesion.
•Skin or soft tissue infection at the site of needle placement.
•Systemic sepsis.
•Frank coagulopathy: Increased risk of spinal epidural hematoma (SEH)
•Recent pharmacologic anticoagulation: Increased risk of SHE
•Uncorrected maternal hypovolemia (Eg: Hemorrhage).
• Thrombocytopenia (Relative contraindication):
Platelet count >75000 Low risk of SEH.
Platelet count 50000-75000 Balance risk and benefit ratio.
Platelet count <50000: Neuraxial technique avoided.
19.
CONSIDERATIONS INSPINAL ANESTHESIA FOR CS:-
Physiological changes.
Pre-op preparations.
Preloading/ co-loading
Anti aspiration prophylaxis
Positioning in RA
Choice of LA
Choice of vasopressors
Complications of RA i.e. Nausea and vomiting, Hypotension,
accidental intravascular injection , PDPH, LA toxicity.
20.
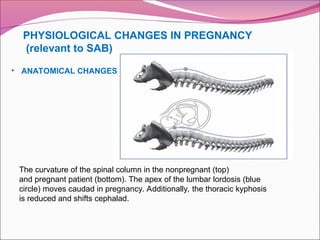
PHYSIOLOGICAL CHANGES INPREGNANCY
(relevant to SAB)
The curvature of the spinal column in the nonpregnant (top)
and pregnant patient (bottom). The apex of the lumbar lordosis (blue
circle) moves caudad in pregnancy. Additionally, the thoracic kyphosis
is reduced and shifts cephalad.
• ANATOMICAL CHANGES
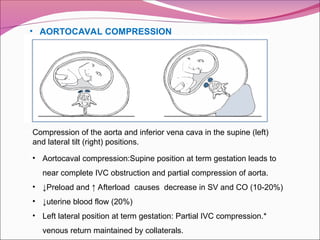
• AORTOCAVAL COMPRESSION
Compressionof the aorta and inferior vena cava in the supine (left)
and lateral tilt (right) positions.
• Aortocaval compression:Supine position at term gestation leads to
near complete IVC obstruction and partial compression of aorta.
• ↓Preload and ↑ Afterload causes decrease in SV and CO (10-20%)
• ↓uterine blood flow (20%)
• Left lateral position at term gestation: Partial IVC compression.*
venous return maintained by collaterals.
23.
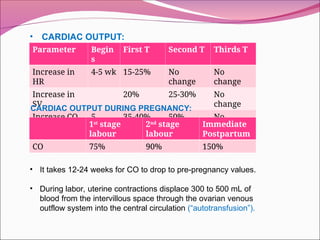
• CARDIAC OUTPUT:
ParameterBegin
s
First T Second T Thirds T
Increase in
HR
4-5 wk 15-25% No
change
No
change
Increase in
SV
20% 25-30% No
change
Increase CO 5
week
35-40% 50% No
change
CARDIAC OUTPUT DURING PREGNANCY:
1st
stage
labour
2nd
stage
labour
Immediate
Postpartum
CO 75% 90% 150%
• It takes 12-24 weeks for CO to drop to pre-pregnancy values.
• During labor, uterine contractions displace 300 to 500 mL of
blood from the intervillous space through the ovarian venous
outflow system into the central circulation (“autotransfusion”).
24.
• Pre-op preparation
History and physical examination, airway and spine examination.
Fasting status:
-Clear liquids (Eg: Water, fruit juices without pulp, carbonated beverages) up to
2 hours before induction of anesthesia.
-Fasting period for solids of upto 6 to 8 hrs depending on the type of food
ingested (Fat content).
Informed consent.
Blood type or cross-matching.
-CS is associated with >500 ml blood loss. Assure blood availability in blood
bank.
-Assess the patient for risk factors of PPH like anemia, twins, adherent placenta
previa etc.
25.
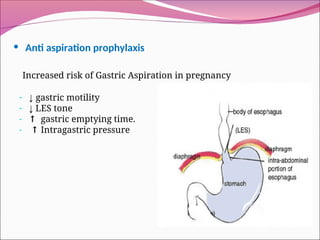
• Anti aspirationprophylaxis
Increased risk of Gastric Aspiration in pregnancy
- ↓ gastric motility
- ↓ LES tone
- ↑ gastric emptying time.
- ↑ Intragastric pressure
26.
Antiaspiration Prophylaxis:
Planned CS:
Tab. Ranitidine 150 mg and Metoclopramide 10 mg PO
night before and 60-90 minutes before surgery
Emergency CS :
• 0.3M Sodium Citrate, 30mL PO 30 Min before Surgery.
• Ranitidine 50 mg IV + Metoclopramide, 10 mg IV prior to
surgery.
27.
Anesthesia machineand monitor check.
Preparation of airway equipment.
Check medication availability (Anesthetics, vasopressors,
uterotonics).
Prophylactic antibiotics:According to 2018 ACOG guidelines,
prophylactic antibiotics within 30 min before incision to reduce the
incidence of post-op endometritis, wound infection and total
maternal infectious morbidity.
Antibiotics with efficacy against gram +ve, & -ve and some
anaerobie bacteria are commonly used for prophylaxis.
Intravenous access: Wide bore IV cannula 16 or 18G.
28.
• PRELOADING /CO-LOADING
Preloading- rapid adminisration of crystalloids (1-
1.5l) prior to initiation of intrathecal injection.
Co-loading- rapid administration of crystalloids(15-20
ml/kg) initiated at the time of intrathecal injection.
Crystalloids/ colloids
Implication – Initiation of anaesthesia should not be delayed in
order to administer a fixed volume of fluid.
29.
• Supplemental oxygen
-Preoxygenationbefore GA.
-Maternal O2 delivery of high Fio (>0.6) may be of benefit
in emergency delivery of compromised fetus.
-Routine administration of supplemental O2 during
elective CS with neuraxial anesthesia of unclear
benefit.
30.
• POSITIONS FORRA
Lateral position
• better uteroplacental
blood flow.
• more comfortable.
• minimizes patient
movement during
needle insertion.
Sitting position
• Distance from skin to
epidural space is
shorter.
• Restricted use : i.e.in
umbilical cord prolapse,
footling presentation.
31.
POSITIONING IN RACont…..
Minimum left lateral tilt of 25º
left lateral displacement to be maintained with a
wedge under the right buttock .
1o cm
34 cm
2.5
cm
32.
Spinal anesthesia forCS
•Most commonly used.
•Rapid onset of dense neuroblockade.
•Technically easier.
•Cost-effective.
•Negligible risk of local systemic anaesthetic toxicity (LAST).
•Minimal drug transfer to fetus.
•Safe to administer in pre-eclampsia.
•Use of pencil-point spinal needles (25 & or smaller) instead of
cutting-bevel spinal needles is recommended to minimize the risk of
PDPH.
•Reduced dose of intrathecal local anesthetic.
•Hyperbaric bupivacaine 10-15 mg most commonly used.
•Intrathecal fentanyl added to improve quality of anesthesia.
•Intrathecal morphine for post-operative analgesia.
33.
Anaesthetic blockade:
Sensory blockof T4 to sacral dermatomes.
The absence of light touch sensation at the T6 level indicates an
adequate block to proceed without pain or discomfort in most
cases.
Dense motor block of lumbosacral plexus (Assessed by straight
leg raise test).
34.
DECREASE IN LOCALANAESTHETIC
REQUIREMENT DURING PREGNANCY
1.↑ Neural susceptibility to LA
2. Epidural plexus engorgement.
3. CSF changes a)↓CSF protein (↑unbound drug)
b)↑ CSF pH (↑ unionised drug)
4. Apex of thoracic kyphosis higher.
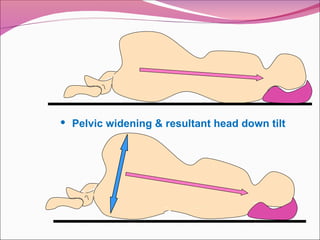
5.Pelvic widening & resultant head down tilt in lateral position.
35.
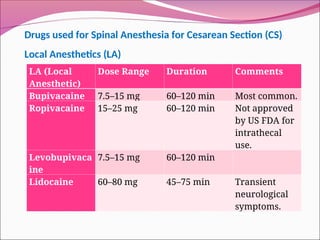
LA (Local
Anesthetic)
Dose RangeDuration Comments
Bupivacaine 7.5–15 mg 60–120 min Most common.
Ropivacaine 15–25 mg 60–120 min Not approved
by US FDA for
intrathecal
use.
Levobupivaca
ine
7.5–15 mg 60–120 min
Lidocaine 60–80 mg 45–75 min Transient
neurological
symptoms.
Drugs used for Spinal Anesthesia for Cesarean Section (CS)
Local Anesthetics (LA)
36.
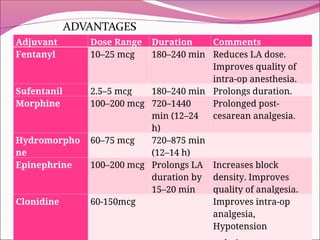
Adjuvant agents
ADVANTAGES
Improvesthe quality of intraoperative
anaesthesia
Prolongs the postoperative analgesia
Reduce the dose of LA and thus the side effects.
37.
Adjuvant Dose RangeDuration Comments
Fentanyl 10–25 mcg 180–240 min Reduces LA dose.
Improves quality of
intra-op anesthesia.
Sufentanil 2.5–5 mcg 180–240 min Prolongs duration.
Morphine 100–200 mcg 720–1440
min (12–24
h)
Prolonged post-
cesarean analgesia.
Hydromorpho
ne
60–75 mcg 720–875 min
(12–14 h)
Epinephrine 100–200 mcg Prolongs LA
duration by
15–20 min
Increases block
density. Improves
quality of analgesia.
Clonidine 60-150mcg Improves intra-op
analgesia,
Hypotension
38.
Complications of neuraxialanesthesia
Hypotension.
Failure of neuraxial blockade.
High block or total spinal
Nausea and vomiting
Pruritis.
Hypothermia and shivering.
39.
HYPOTENSION
• Most commonsequela of neuraxial anesthesia.
• Neuraxial anesthesia----- sympathetic blockade---- vasodilation with
modest degree of venodilation → decrease in SVR
• Leads to compensatory increase in HR and SV------Cardiac output
increases. (Secondary response).
• Systolic blood pressure <100 mmHg or fall of 20% from baseline).
• Consequences of hypotension:
-Nausea and vomiting.
-Dizziness, decreased level of consciousness
-Impairment of uteroplacental perfusion with fetal hypoxia and acidosis.
40.
Prevention & treatmentof hypotension:
•Left uterine displacement (15 degree tilt recommended): By providing
table tilt or wedge under right hip.
•Leg elevation or compression (Helpful in low resource setting).
•Intravenous fluid (No evidence based recommendation):
Crystalloid preload has no benefit over crystalloid co-load.
Colloid preload is more effective than crystalloid preload.
Colloid preload & co-load are more effective than crystalloid co-load.
Colloids are high cost and potential adverse effects, hence not used
routinely.
Consider crystalloid co-loading.
41.
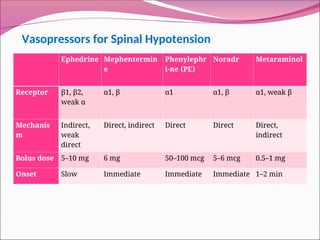
Vasopressors for SpinalHypotension
Ephedrine Mephentermin
e
Phenylephr
i-ne (PE)
Noradr Metaraminol
Receptor β1, β2,
weak α
α1, β α1 α1, β α1, weak β
Mechanis
m
Indirect,
weak
direct
Direct, indirect Direct Direct Direct,
indirect
Bolus dose 5–10 mg 6 mg 50–100 mcg 5–6 mcg 0.5–1 mg
Onset Slow Immediate Immediate Immediate 1–2 min
42.
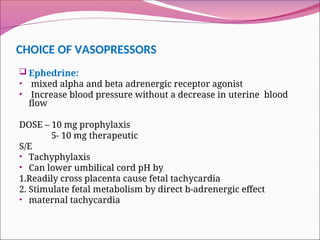
CHOICE OF VASOPRESSORS
Ephedrine:
• mixed alpha and beta adrenergic receptor agonist
• Increase blood pressure without a decrease in uterine blood
flow
DOSE – 10 mg prophylaxis
5- 10 mg therapeutic
S/E
• Tachyphylaxis
• Can lower umbilical cord pH by
1.Readily cross placenta cause fetal tachycardia
2. Stimulate fetal metabolism by direct b-adrenergic effect
• maternal tachycardia
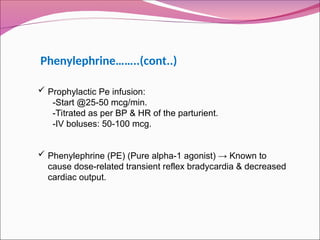
Prophylactic Peinfusion:
-Start @25-50 mcg/min.
-Titrated as per BP & HR of the parturient.
-IV boluses: 50-100 mcg.
Phenylephrine (PE) (Pure alpha-1 agonist) → Known to
cause dose-related transient reflex bradycardia & decreased
cardiac output.
Phenylephrine……..(cont..)
45.
Norepinephrine (NE)
Mild beta1+alpha1agonist action: Less bradycardia and less
CO.
Prophylactic NE infusion:
5 mcg/mlStart @30 ml/hr.Titrated 0-60 ml/hr.
Iv boluses: 5-6 mcg/mlNe infusion is as effective as
phenylephrine in maintaining BP.
Bradycardia is less likely.
Effects on fetal transfer & metabolic effects is also not clear
46.
Best management ofspinal hypotension:
Measure accurate baseline systolic arterial pressure (SAP).
Calculate values for 80% & 90% of baseline SAP.
A prophylactic infusion of phenylephrine should be started immediately after
injection of the spinal anesthetic.
Starting rate at 15-30 ml/h of 100 mcg/ml concentration (25-50 mcg/ min).Can be
titrated by 5-10 ml/h in response to hypotension/hypertension.If SAP < 80%, then
100 mcg rescue boluses should be given.
Use LUD with at least 15 degree pelvic tilt and a free-flowing crystalloid co-load
(15 ml/kg or 1000 ml) immediately after spinal injection.
Measure BP every 1-2 min after spinal injection.
Maintain BP near baseline. Avoid a decrease to <80% baseline.
47.
Hypotension combinedwith a low HR should be treated with ephedrine 3-6
mg if SAP <90%
For hypotension with bradycardia (SAP <80% baseline & HR <60
beats/min), an anticholinergic drug (Glycopyrrolate or atropine) may be
required.
After delivery, the phenylephrine may be weaned rapidly over
approximately 5 min. Oxytocin & carbetocin may precipitate further
hypotension.
In resource-limited environments, boluses of phenylephrine (50-100 mcg),
ephedrine (10 mg), metaraminol (0.5 mg), or adrenaline (10 mg) are
recommended to keep SAP >90% baseline & HR <120% baseline.
CONT…
48.
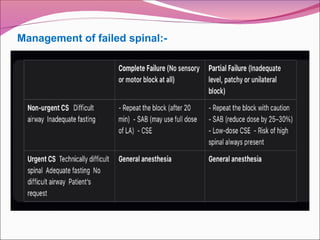
Failure ofneuraxial blockade
Neuroblockade insufficient in extent, density, or duration to provide
anesthesia for CS.
Causes of failure:
Inadequate dose.
Wrong drug.
Misplaced injectate.
Faulty technique.
Blocked needle.
Inappropriate positioning.
Anatomical deformities.
Kyphosis/scoliosis.
Obesity
After skin incision:
Ivfentanyl boluses (25-50 mcg).
IV ketamine 5-10 mg boluses.
Inhaled NO (40-50% in oxygen).
General anesthesia.Wound infiltration with LA.
Reassurance, communication & documentation.
Avoid excessive sedation.
Accept failure.
Reassurance.
Communication.
Documentation.
51.
Regional Anaesthesia –Complications
High Spinal Anaesthesia:
Rostral spread of intrathecal dose, or Inadvertent
intrathecal administration of epidural dose.
Clinical Features:
Complete motor and sensory palsy,
Hypotension, Bradycardia,
Unconsciousness,
Loss of protective airway reflexes,
respiratory arrest
Treatment: Prompt tracheal intubation and ventilation
with 100% oxygen, maintenance of maternal circulation
52.
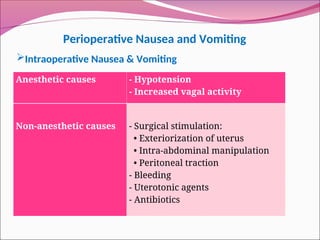
Regional Anaesthesia –Complications
NAUSEA AND VOMITING
CAUSES –
1.Hypotension
hypotension
Gut ischemia brain stem hypoperfusion
Release of emetogenic Stimulation of vomiting
Substance Centre
Vomiting
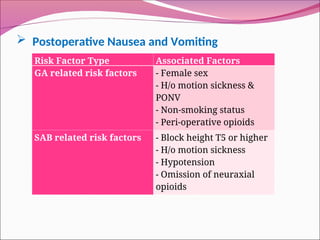
Postoperative Nauseaand Vomiting
Risk Factor Type Associated Factors
GA related risk factors - Female sex
- H/o motion sickness &
PONV
- Non-smoking status
- Peri-operative opioids
SAB related risk factors - Block height T5 or higher
- H/o motion sickness
- Hypotension
- Omission of neuraxial
opioids
55.
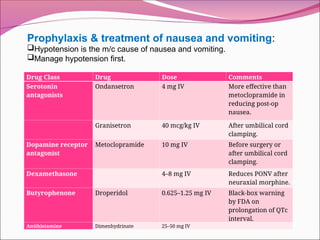
Prophylaxis & treatmentof nausea and vomiting:
Hypotension is the m/c cause of nausea and vomiting.
Manage hypotension first.
Drug Class Drug Dose Comments
Serotonin
antagonists
Ondansetron 4 mg IV More effective than
metoclopramide in
reducing post-op
nausea.
Granisetron 40 mcg/kg IV After umbilical cord
clamping.
Dopamine receptor
antagonist
Metoclopramide 10 mg IV Before surgery or
after umbilical cord
clamping.
Dexamethasone 4–8 mg IV Reduces PONV after
neuraxial morphine.
Butyrophenone Droperidol 0.625–1.25 mg IV Black-box warning
by FDA on
prolongation of QTc
interval.
Antihistamine Dimenhydrinate 25–50 mg IV
56.
Most commonside effect after intrathecal & epidural opioids.
Higher incidence and severity after intrathecal opioids.
Mediated through central µ-opioid receptors, unrelated to histamine
release. Generalized or localized to nose, face and chest.
Dose dependent, self-limiting.
Prophylaxis: 5-HT3 receptor antagonist (Ondansetron 4-8 mg)
PRURITIS
57.
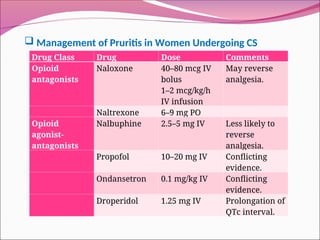
Management ofPruritis in Women Undergoing CS
Drug Class Drug Dose Comments
Opioid
antagonists
Naloxone 40–80 mcg IV
bolus
1–2 mcg/kg/h
IV infusion
May reverse
analgesia.
Naltrexone 6–9 mg PO
Opioid
agonist-
antagonists
Nalbuphine 2.5–5 mg IV Less likely to
reverse
analgesia.
Propofol 10–20 mg IV Conflicting
evidence.
Ondansetron 0.1 mg/kg IV Conflicting
evidence.
Droperidol 1.25 mg IV Prolongation of
QTc interval.
58.
Regional Anaesthesia –Complications
Post Dural Puncture Headache
Risk factors:
• Age<40
• Women
• Pregnancy
• Use of wider guage and dura cutting spinal needle.
Symptoms:
• Frontal / Occipital headache
• Positional
• Varying severity
• Neck Stiffness
• Onset within 48 hours
Hypothermia andshivering
Common after neuraxial anesthesia.
Vasodilation-induced core-to-periphery heat redistribution.
Impairment of centrally mediated thermoregulatory contral.
Peri-operative adverse outcomes :Wound infection.Coagulopathy.Increased
blood loss.Increased O2 consumption, prolonged recovery.
Prevention & treatment:
Forced air warming.
Increase OT temperature from 20° C to 23° с.
Pethidine 12.5-25 mg IV: most effective.
Clonidine 150 mcg.
Dexmedetomidine 0.5 mcg/kg.} concerns regarding hypotension and
sedation
61.
SPINAL ANESTHESIA FORLSCS IN SPECIAL DISEASE CONDITIONS
Pre-eclampsia
Major concerns:- Hypertension and Thrombocytopenia
Thrombocytopenia:
Spinal/epidural anaesthsia causes bleeding or spinal epidural hematoma.
Risk of failed intubation during GA for C-section : I in 443.
Failed intubation in obstetrics is 8 times higher than non-obstetric patients.
Incidence of spinal Epidural Hematoma (SEH) in general population: very low.
Incidence of SEH in Obstetric patients: Lower than non-obstetric patients.
Incidence of epidural hematoma after neuraxial techniques in Obstetrics: 1 in
2,00,000 to 1 in 2,50,000.
63.
Platelet transfusion:
No evidenceto assess correct platelet transfusion threshold prior to
neuraxial techniques.
Consider risks of platelet transfusion.
ACOG recommends platelet transfusion in preeclampsia for active
bleeding or to improve the platelet count to 50,000 x 106/L before
Cesarean delivery.
64.
Safe practice inthrombocytopenia:
Consider trend of thrombocytopenia, rather than just a number.
Rule out coagulopathy .
With platelet counts <70000, make an individual decision based on risks
and benefits of neuraxial vs GA.
A single-shot spinal technique may be preferable to an epidural technique
because of the smaller needle size.
The most skilled anesthesia, provider should perform the neuraxial
procedure.
Check platelet count for evidence of a return toward normal measurements
before removal of the epidural catheter.
Monitor the patient after delivery for neurological signs suggestive of SHE.
65.
Hypertension:
Historical belief:-
Spinal anesthesiain patients with severe preeclampsia causes severe hypo-
tension and decreased uteroplacental perfusion.
Prevented widespread use of spinal anesthesia and favored general anes-
thesia in Pre-eclampsia.
Current evidence suggests:-
Parturients with severe pre-eclampsia experience less frequent, less severe
hypotension than healthy parturients.
Require smaller doses of vasopressors than normotensives.
Spinal anesthesia, can be safely given in severe preeclampsia for Cesarean
delivery.
66.
Challenges:
Poorly controlled hypertensionand seizures.
Hypertensive response to laryngoscopy.
Raised intracranial pressure.
Airway edema/tongue bite.
Bleeding :-Thrombocytopenia/coagulopathy.
Depleted intravascular volume.
Risk of pulmonary edema and end organ dysfunction.
Drug interaction with magnesium sulfate:- uterine atony, increased risk of
PPH, prolong neuromuscular block.
SPINAL ANESTHESIA FOR LSCS IN
ECLAMPSIA
67.
Choice of anaesthesiain patient with Eclampsia:
Fully conscious, alert, seizure free: Neuraxial anesthesia.
Persistent coma, localizing signs,seizures, s/o raised ICP:
General anesthesia.
Considerations for neuraxial anaesthesia:-
Thrombocytopenia/coagulopathy:- platelet >70,000, no
coagulopathy, no bleeding Go for spinal.
Hypotension not a concern.
Judicious use of fluids.
vasopressors to be used to prevent hypotension.
68.
SPINAL ANESTHESIA FORLSCS IN ANTEPARTUM HAEMORRHAGE
PLACENTA PREVIA AND PLACENTAL ABRUPTION
Anaesthetic management:
Choice of technique depends on:
Indication/urgency of delivery: Elective/emergency caesarian/acute fetal
distress.
Severity of maternal hypovolemia: Bleeding/shock/stable.
Obstetric history: H/o previous caesarian delivery.
1. Emergency CS/placenta previa with active bleeding:
General anesthesia preferred.
69.
2. For electiveCS/placenta previa without bleeding:
Neuraxial techniques is safe:
Combined spinal epidural/Epidural to allow extension for unexpected
cesarean hysterectomy.
Plan in place to convert to general anaesthesia in case of massive PPH.
Preparations:
Wide bore IV cannula kept ready.
Resuscitative measures and blood loss.
Warm IV fluids.
Uterotonics.
Cross matched blood.
Consent for general anaesthesia.
Aspiration prophylaxis.
70.
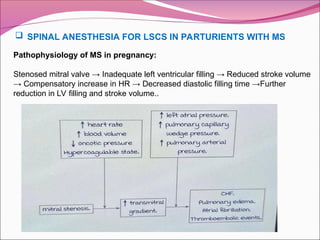
Pathophysiology of MSin pregnancy:
Stenosed mitral valve → Inadequate left ventricular filling → Reduced stroke volume
→ Compensatory increase in HR → Decreased diastolic filling time →Further
reduction in LV filling and stroke volume..
SPINAL ANESTHESIA FOR LSCS IN PARTURIENTS WITH MS
72.
vi. Prevent/monitor forpulmonary edema:
Careful fluid balance.
Continuous pulse oximetry throughout labor & postpartum.
Recognize & treat hypertensive disorders of pregnancy.
vii Manage pulmonary edema:
Consider diuresis.
Administer supplemental oxygen.
Labor in upright position.
If necessary, consider intubation & controlled ventilation with PEEP.
Viii. Postpartum monitoring: monitor for postpartum pulmonary edema.
73.
Predelivery planning &preparation:
Summarize cardiac, obstetric and anesthesia history & risk factors.
Have a clear plan of management.
Risk stratification according to mWHO criteria.
Optimize anticoagulation regime to facilitate neuraxial techniques.
Multidisciplinary planning of labor & delivery by the pregnancy heart team.
Determine delivery plan between 20-30 weeks of gestation:
Timing (Induction vs spontaneous labor).
Mode of delivery (vaginal/operative).
Delivery location.
Possible need for cardiac monitoring.
Postpartum plans for monitoring.
74.
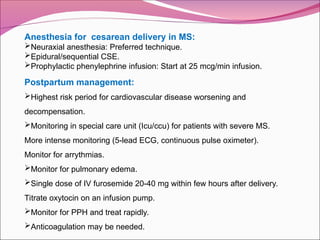
Anesthesia for cesareandelivery in MS:
Neuraxial anesthesia: Preferred technique.
Epidural/sequential CSE.
Prophylactic phenylephrine infusion: Start at 25 mcg/min infusion.
Postpartum management:
Highest risk period for cardiovascular disease worsening and
decompensation.
Monitoring in special care unit (Icu/ccu) for patients with severe MS.
More intense monitoring (5-lead ECG, continuous pulse oximeter).
Monitor for arrythmias.
Monitor for pulmonary edema.
Single dose of IV furosemide 20-40 mg within few hours after delivery.
Titrate oxytocin on an infusion pump.
Monitor for PPH and treat rapidly.
Anticoagulation may be needed.
75.
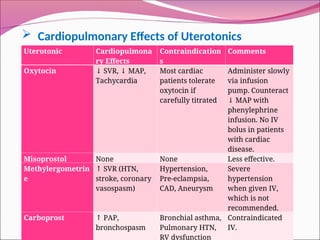
Cardiopulmonary Effectsof Uterotonics
Uterotonic Cardiopulmona
ry Effects
Contraindication
s
Comments
Oxytocin ↓ SVR, MAP,
↓
Tachycardia
Most cardiac
patients tolerate
oxytocin if
carefully titrated
Administer slowly
via infusion
pump. Counteract
MAP with
↓
phenylephrine
infusion. No IV
bolus in patients
with cardiac
disease.
Misoprostol None None Less effective.
Methylergometrin
e
↑ SVR (HTN,
stroke, coronary
vasospasm)
Hypertension,
Pre-eclampsia,
CAD, Aneurysm
Severe
hypertension
when given IV,
which is not
recommended.
Carboprost ↑ PAP,
bronchospasm
Bronchial asthma,
Pulmonary HTN,
RV dysfunction
Contraindicated
IV.
76.
References:
Chestnut DH, WongCA, Tsen LC, et al. Chestnut’s Obstetric
Anesthesia: Principles and Practice. 6th ed. Philadelphia:
Elsevier; 2020.
Miller RD, et al. Miller’s Anesthesia. 9th ed. Philadelphia:
Elsevier; 2020.
ISA Kerala Online Classes. Anaesthesia for Cesarean Section:
Safe Practices [online lecture]. Indian Society of
Anaesthesiologists, Kerala State Chapter; [Accessed 2022 sep
12]
#5 Before we proceed to the anaesthetic management, we must know the complications associated with the procedure
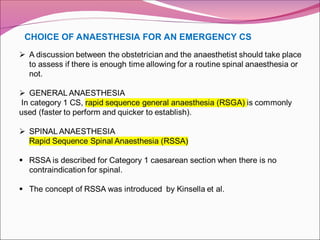
#9 The surgical indication and therefore the speed of delivery. Anaesthetic considerations include the presence of an epidural catheter, the anticipation of difficult airway, contraindications to regional techniques or potential technical difficulties like spinal deformity and maternal preference.
If time not a factor, RA is preferred for both planned and semi emergency situations
Emergency cases without anticipated difficult airway, SAB is given
If Epidural catheter for labour analgesia in situ, block extended to levels adequate for caesarean
In Fetal Distress, Subarachnoid block is safe. Even if hypotension occurs, fetal circulation isn’t compromised
If speed of delivery is of essence, RA is contraindicated or in severe maternal haemorrhage GA is administered.
#15 The rationale for RSSA:Urgency in category 1 cesarean sections: In emergent situations, the time to deliver the baby is critical, and RSSA aims to minimize the time spent on anesthesia preparation. Reducing complications: By reducing the time to anesthesia, the risk of complications associated with prolonged general anesthesia, such as aspiration, can be minimized. Optimizing fetal oxygenation: Rapid anesthesia can help optimize fetal oxygenation in emergencie
#19 Before we move to the conduct of RA or GA , we would like to discuss the considerations under RA or GA
#26 Na citrate does not dercrease the volume and dose need to be repeated if the surgery is prolonged .
#28 Role of i.v fluids: decrease the frequency of neuraxial anaesthesia associated hypotension.
Role of i.v fluids: decrease the frequency of neuraxial anaesthesia associated hypotension.
A balanced salt solution – ringer lactate is preferred
#48 During cesarean section under neuraxial anesthesia, pain has replaced accidental awareness under general anesthesia as the most common successful medicolegal claim against obstetric anesthetists in the uk
#58 Post Dural Puncture Headache
Frontal or Occipital headache. Severity varies – Mild to debilitating.
Symptoms worse when upright. Relieved in supine.
Onset in first 48 hours. Last less than a week
#59 2 people will wash up.
Sumatirptan is a serotonin agonist with cerebral vasoconstrictor action. Given s/c


![References:
Chestnut DH, Wong CA, Tsen LC, et al. Chestnut’s Obstetric
Anesthesia: Principles and Practice. 6th ed. Philadelphia:
Elsevier; 2020.
Miller RD, et al. Miller’s Anesthesia. 9th ed. Philadelphia:
Elsevier; 2020.
ISA Kerala Online Classes. Anaesthesia for Cesarean Section:
Safe Practices [online lecture]. Indian Society of
Anaesthesiologists, Kerala State Chapter; [Accessed 2022 sep
12]](https://image.slidesharecdn.com/spinalanesthesiainparturientsforcesareansection-250526111744-459f727a/85/spinal-anesthesia-in-parturients-for-cesarean-section-ppt-76-320.jpg)



























![Obstetric Anesthesia ppt [ Natnael Dechasa ].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obstetricanesthesiapptnatnaeldechasa-230310124013-7b6867cb-thumbnail.jpg?width=640&height=640&fit=bounds)



























































