INTRODUCTION
Postural headachesfollowing intervention that disrupts
meningeal integrity are most commonly labelled post dural
puncture headaches.
First described by August Beir and classically presents as a
postural headache following therapeutic or diagnostic
intervention of the epidural or spinal space.
3.
Incidence varies,estimated to be 36% or more following lumber
puncture , 0-10%following spial anaesthesia and 81% following
accidental dural puncture during epidural insertion.
Rates of accidental dural puncture during epidural insertion in
pregnancy are estimated to be 0.04%- 6% and up to 50-80%
patient with ADP develop PDPH.
Normal CSF volume- 150ml
CSF pressure -5-15 cmH2O, increases to 40cm in upright
position.
4.
Pathogenesis
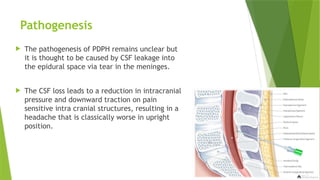
The pathogenesisof PDPH remains unclear but
it is thought to be caused by CSF leakage into
the epidural space via tear in the meninges.
The CSF loss leads to a reduction in intracranial
pressure and downward traction on pain
sensitive intra cranial structures, resulting in a
headache that is classically worse in upright
position.
5.
Traction onneural tissue precipitates symptoms from pain-
sensitive structures, eg, the meninges, blood vessels, cranial
nerves, and upper cervical nerves.
Displacement of the brain downward when the patient is in the
upright position contributes to orthostatic symptoms.
Secondly, the loss of CSF produces a compensatory
venodilatation ( the Monro Kellie doctrine).
The Monro Kellie doctrine, or hypothesis, states that the sum of
volumes of the brain tissue, CSF, and intracranial blood is
constant.
The consequence of a decrease in CSF volume is a
compensatory increase in blood volume.
The venodilatation is then responsible for the headache.
6.
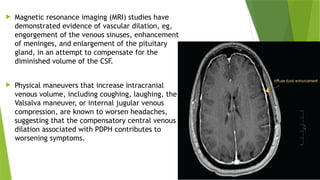
Magnetic resonanceimaging (MRI) studies have
demonstrated evidence of vascular dilation, eg,
engorgement of the venous sinuses, enhancement
of meninges, and enlargement of the pituitary
gland, in an attempt to compensate for the
diminished volume of the CSF.
Physical maneuvers that increase intracranial
venous volume, including coughing, laughing, the
Valsalva maneuver, or internal jugular venous
compression, are known to worsen headaches,
suggesting that the compensatory central venous
dilation associated with PDPH contributes to
worsening symptoms.
7.
Clinical Presentation
ONSET:-
Onset of symptoms is generally delayed, with headache usually
beginning 12-48 hrs and rarely more than 5 days following
meningeal puncture.
An onset of symptoms within 1 hour of neuraxial procedures is
suspicious for pneumocephalus , especially in the setting of an
epidural loss of resistance technique using air.
8.
Presentation :-
The cardinal feature of PDPH is its postural nature, with
headache symptoms worsening in the upright position and
relieved or at least improved with recumbency.
The international headache society (IHS) diagnostic criteria
further describe this positional quality as worsening within 15
min of setting or sitting and improving within 15 min after
lying.
Headache is always bilateral, with distribution that is frontal
(25%), occipital (27%), or both (45%).
Dull aching, throbbing or pressure type.
9.
Although thereis no universally accepted severity scale, one
practical approach is to have patients simply rate their
headache intensity using 10 point analogue, with scale of
1-3 -> mild
4-6 -> moderate
7-19 -> severe
10.
Associated Symptoms
HIScriteria for PDPH areas follows :
Headache , accompanied by at least one of these symptoms:
Neck stiffness
Tinnitus
Hypoacusia
Photophobia
Nausea
11.
Risk Factor
PatientCharacteristics :
Age : it is uncommon in patients less than 10 years of age
Peak incidence is in the teens and early 20s.
Gender : non pregnant females have twice the risk compared to
age matched men.
Pregnancy
BMI
Patients with others form of headache
Prev history of PDPH
Prev history of ADP
12.
Procedural details:
Needle size
Needle tip design (cutting vs noncutting)
Insertion of cutting needles with bevel parallel to the long axis of
the spine
Experience, comfort, skill of the operator
A number of procedural details do not appear to influence the
rate of development of PDPH including-
patient position at the time of meningeal puncture
bloody tap during spinal anaesthesia
Addition of opiates
Volume of CSF removed
13.
Prevention
General measures:
Appropriate patient selection
Practitioners
Use of ultrasound
Bed rest
Aggressive oral and intravenous hydration
Caffeine
14.
Spinal Technique:
Needle selection
Replacing the stylet after CSF collection but prior to needle
withdrawal
Continuous spinal anesthesia
Intravenous aminophylline
Epidural Technique :
Using smallest feasible epidural needles
Air vs liquid for identification of epidural space
Bevel orientation for epidural needle insertion remains a
matter of debate
Diagnosis and DifferentialDiagnosis
Remains a diagnosis of exclusion, although headache following
meningeal puncture will naturally be suspected to be PDPH, it
remains critical to rule out other etiologies.
While postpartum headaches occur in up to 40% of postpartum
women ; 50-70% are tension type or migraine; only 5-15% are
PDPH.
Importantly, one study found that 24% of postpartum headaches
were due to preeclampsia.
Other cause like Medication related headaches also be
excluded.
17.
Careful history:
Known or possible meningeal puncture
Delayed onset of symptoms (but within 48hrs)
Bilateral postural headache
Possibly accompanied by associated symptoms if moderate or
severe.
Physical examination :
Plays limited role in the diagnosis of PDPH
Vital sign ( normal BP and absence of fever)
Basic neurologic exam should be documented ( gross motor ans
sensory function plus ocular and facial movements)
18.
Firm bilateraljugular venous pressure applied briefly (10-15 sec)
tends to worsens headaches secondary to intracranial
hypotension.
Conversely sitting epigastric pressure test may result in transient
relief from symptoms (Gutsche sign),
Patient is placed in sitting position until headache symptoms
manifest. Firm continuous pressure applied with one hand on the
abdomen and other hand at the back of the patient.
Symptoms relieved within 15-30sec of pressure and resumes once
pressure released.
Skin over epidural or spinal puncture site should be inspected for
inflammation and tenderness.
19.
Investigation :
Lab studies are usually not necessary for the diagnosis of PDPH.
LP may reveal lower opening pressure and increase CSF protein.
MRI with gadolinium contrast however reveals changes.
Two key finding using T1 weighted contrast MRI are; meningeal
enhancement and descent or sagging of the brain.
Treatment
Once thediagnosis of PDPH made, patient should be provided
explanation of presumed etiology, anticipated natural course
and treatment options.
Treatment are the forms of:
Conservative management
Pharmacological management
Invasive management
23.
Conservative Management
Reassurance: in untreated patients a median duration of
symptoms of 5 days with a range of 1-12 days.
Bed rest
Oral and intravenous hydration
Abdominal binders
24.
Pharmacological Management
Analgesics:
Acetaminophen (1gm 8hrly), NSAID (ibuprofen 600mg 6hrly),
opiates etc.
Methylxanthines :
These includes aminophylline(3-5mg/kg iv), theophylline (200-
300mg BD) and caffeine
Caffeine is thought to treat by inducing cerebral
vasoconstriction, with dose range from 75mg – 500mg orally and
intravenously one time and repeated.
Caffeine is associated with cardiac arrythmias, seizures and high
dose may enter into the breast and cause neonatal irritability.
25.
Corticosteroidogenics :
Corticotropins and its synthetic analogues (cosyntropin(1mg iv),
tetracosactrin(250mcg iv).
Postulated mechanism include CSF retention through
mineralocorticoid-mediated sodium reabsorption and direct
analgesic effect via its glucocorticoid activity.
Corticosteroids, Similar to corticosteroidogenics, corticosteroids
have multiple physiologic effects that could theoretically
improve symptoms of PDPH, Hydrocortisone (200 mg IV initially,
followed by 100 mg every 8 hours for 6 doses)
Serotonin type 1d receptor agonists :
These agents cause cerebral vasoconstriction and are commonly
used for migraine headache. Despite anecdotal reports of
success, sumatriptan(50-100mg) was ineffective for treatment
of severe PDPH in a small randomized, prospective study.
26.
Ergot alkaloids:
These cerebral vasoconstrictive agents are also commonly used
for migraine headache. A small, uncontrolled pilot study
suggested that methylergonovine (0.25 mg orally three times
daily for 24–48 hours) may hasten resolution of PDPH.
Anticonvulsants:
Several membrane-stabilizing agents are widely used for various
pain syndromes. Gabapentin (200 mg initially, followed by 100–
300 mg three times daily, with dose adjusted to tolerance and
efficacy).
Pregabalin (75 mg twice a day for 2 days, then 150 mg twice a
day for 2 days) was demonstrated to result in lower pain scores
and analgesic consumption in patients with PDPH following
spinal anesthesia or LP
Epidural saline:
Epidural saline, as bolus and infusion, has a long history of use
for treatment of PDPH.
Bolus injections of epidural saline (usually 20–30 ml, repeated as
necessary if a catheter is present) have been reported to
produce prompt and virtually universal relief of PDPH, yet the
practice is plagued by an extremely high rate of headache
recurrence.
This transient effect is not surprising as increases in epidural
pressure following bolus administration of saline have been
demonstrated to return to baseline within 10 minutes.
Favorable results achieved with this approach have been
speculated to represent the mechanical re-approximation of a
dural flap (the “tin-lid” phenomenon).
However, bolus administration of saline for treatment of PDPH
has been convincingly shown to be inferior to the EBP, especially
when headaches are secondary to large-bore needle punctures.
29.
Epidural bloodpatch :
After the observation that patients with bloody spinal taps at
lumber puncture were less likely to develop PDPH.
First EBP was performed in 1960, just 2ml of blood was injected
during first EBP and symptoms were relieved.
EBP involves the injection of autologous blood into the epidural
space.
The mechanism of action of EBP, appears to be related to the
ability to stop further CSF loss by the formation of clot over the
defect in the meninges as well as tamponade effect with
cephalad displacement of CSF (epidural pressure patch).
32.
An EBPshould be performed by two personnels.
Contraindication: patient refusal, coagulopathy and sepsis.
Timing of EBP performance is somewhat controversial , with
limited evidence pointing to less failure when performed more
than 48 hrs after PDPH onset.
Volumes of between 2-60ml of blood have been described in
literature.
Standard volume used is 20ml.
Most anaesthesiologist recommend the patient lie flat for 1-2
hrs after the procedure and avoid heavy lifting for 48 hrs.
33.
Safety :
Strict asepsis must be maintained during an EBP.
Do not perform in the presence of leucocytosis or fever dure to
the risk of meningitis.
Minor complication- backache, neck ache and transient
bradycardia.
Major complication are rare and include meningitis , subdural
haematoma, seizures, arachnoiditis and dural puncture.
If an EBP fails to relieve a PDPH, it may be prudent to consider
head imaging to exclude other pathology prior to repeat EBP.
34.
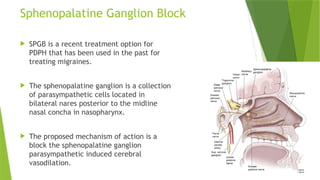
Sphenopalatine Ganglion Block
SPGB is a recent treatment option for
PDPH that has been used in the past for
treating migraines.
The sphenopalatine ganglion is a collection
of parasympathetic cells located in
bilateral nares posterior to the midline
nasal concha in nasopharynx.
The proposed mechanism of action is a
block the sphenopalatine ganglion
parasympathetic induced cerebral
vasodilation.
35.
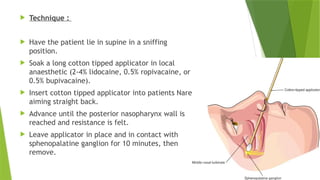
Technique :
Have the patient lie in supine in a sniffing
position.
Soak a long cotton tipped applicator in local
anaesthetic (2-4% lidocaine, 0.5% ropivacaine, or
0.5% bupivacaine).
Insert cotton tipped applicator into patients Nare
aiming straight back.
Advance until the posterior nasopharynx wall is
reached and resistance is felt.
Leave applicator in place and in contact with
sphenopalatine ganglion for 10 minutes, then
remove.
36.
Adverse events:
Nausea
Bitter taste
Discomfort during insertion of applicator
Nasal or throat pain.
37.
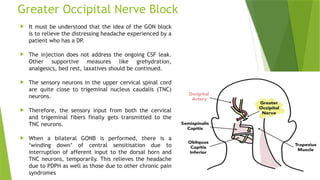
Greater Occipital NerveBlock
It must be understood that the idea of the GON block
is to relieve the distressing headache experienced by a
patient who has a DP.
The injection does not address the ongoing CSF leak.
Other supportive measures like grehydration,
analgesics, bed rest, laxatives should be continued.
The sensory neurons in the upper cervical spinal cord
are quite close to trigeminal nucleus caudalis (TNC)
neurons.
Therefore, the sensory input from both the cervical
and trigeminal fibers finally gets transmitted to the
TNC neurons.
When a bilateral GONB is performed, there is a
‘winding down’ of central sensitisation due to
interruption of afferent input to the dorsal horn and
TNC neurons, temporarily. This relieves the headache
due to PDPH as well as those due to other chronic pain
syndromes
38.
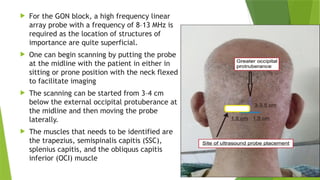
For theGON block, a high frequency linear
array probe with a frequency of 8–13 MHz is
required as the location of structures of
importance are quite superficial.
One can begin scanning by putting the probe
at the midline with the patient in either in
sitting or prone position with the neck flexed
to facilitate imaging
The scanning can be started from 3–4 cm
below the external occipital protuberance at
the midline and then moving the probe
laterally.
The muscles that needs to be identified are
the trapezius, semispinalis capitis (SSC),
splenius capitis, and the obliquus capitis
inferior (OCI) muscle
39.
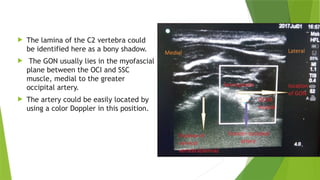
The laminaof the C2 vertebra could
be identified here as a bony shadow.
The GON usually lies in the myofascial
plane between the OCI and SSC
muscle, medial to the greater
occipital artery.
The artery could be easily located by
using a color Doppler in this position.
40.
When to seekfurther consultation?
Symptoms have failed to resolve after an arbitrary duration (7-10
days) or number of EBP (usually 2-3)
Serious non PDPH is suspected or can not reasonably be ruled out.
Lateralizing neurologic signs, fever / chills, seizures or change in
menta status are not consistent with a diagnosis of PDPH or benign
headache
Any headache with atypical features
Headaches that worsens over time and no longer have a positional
nature.


















































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)








