BACKGROUND
• Neuraxial anesthesiahas been performed safely in pediatric
patients for over a century, starting with successful reports of spinal
anesthesia by Bier in an 11-year-old child for thigh tumor resection
in 1898 and by Bainbridge in a 3-month-old infant for strangulated
hernia in 1900.
• Caudal epidural blockade was the next advancement, and by 1954
neuraxial anesthesia had expanded to include a case series of
lumbar epidural anesthetics for inguinal hernia repair in infants and
children.
• As the safety of general anesthesia improved, interest in pediatric
neuraxial anesthesia waned until a resurgence in the mid 1980s
when spinal anesthesia was touted as a safe alternative to general
anesthesia to reduce the risk of post-operative apnea for premature
infants ≤60 weeks post-menstrual age (PMA).
3.
General Anaesthesia VsCentral
Neuraxial Block ??
• Regional anaesthesia and analgesia have been shown to offer
multiple benefits over general anaesthesia and systemic (including
opioid) analgesia.
• Historical concerns over additional risk posed by needle-related
nerve injury have been progressively diluted by the evolution of
ultrasound-guided techniques and the publication of big-data
studies establishing the low incidence of serious complications of
paediatric regional anaesthesia in the modern era.
• These factors, weighed against concerns over the effect of general
anaesthesia on the developing brain and the serious adverse events
associated with the administration of opioids, mean that paediatric
regional anaesthesia remains at the forefront of the perioperative
care of children.
4.
Safety of GAin pediatric age
group??
• Preclinical data suggest that general anaesthetics potentially promote
neuroapoptosis, and there is conflicting evidence from several cohort
studies that young children exposed to volatile anaesthesia might have
demonstrable deficits in subtle neurodevelopmental outcomes.
• It should be noted that the most methodologically robust studies
(accounting for the confounding effects of surgery, pathology, and co-
morbidity) have failed to substantiate this assertion.
• However, concerns persist regarding the dose and time-dependent
neurodevelopmental consequences from both volatile and i.v. anaesthetic
agents during the critical period of synaptogenesis and central myelination.
• Regional anaesthesia permits the dose reduction or even elimination of
general anaesthesia, and the reduction of the adverse effects and events
associated with opioid analgesia.
6.
Neuraxial anaesthesia
• Concernsregarding general anaesthetic-induced cognitive
deficits in patients aged <3 months and the steady prevalence of
lung disease of prematurity mean that neuraxial anaesthesia for
infants retains its place in the armamentarium of the paediatric
anaesthetist.
• Spinal anaesthesia has been shown to be equivalent to general
anaesthesia in terms of neurodevelopmental outcomes in infants,
and there are advantages to using the intrathecal technique
especially in cases of respiratory impairment.
• In paediatric practice, the neuraxis can be accessed and
anaesthetised via two routes:
• intrathecal or epidural (thoracic, lumbar, or caudal).
7.
Advantages of centralneuraxial anaesthesia over general anaesthesia
include
• improved postoperative pain outcomes,
• attenuation of the inflammatory and stress response to surgery,
• avoidance of airway manipulation and interference with
spontaneous ventilation (especially relevant in the event of
increased airway reactivity or pre-existing respiratory impairment),
• cardiovascular stability,
• reduced need for postoperative ventilation,
• reduced paralytic ileus.
8.
Anatomy and Physiology
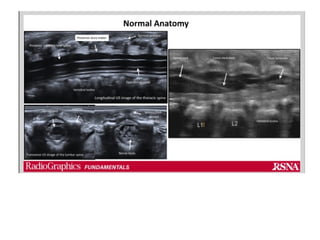
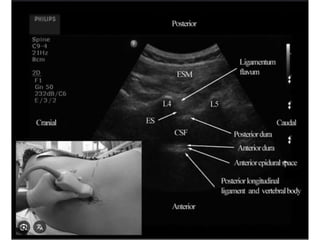
•The anatomy of the vertebra and the relative position of spinal cord
placement in the vertebral canal varies with age.
• Classical literature states that the spinal cord ends (conus
medullaris) are as low as the L3 vertebra in infants, compared to
L1 in adults.Adult levels are reached at about 6 years of age.
• Recent imaging studies have revealed a median level of L2 for
termination of the spinal cord in infants.
• This is essential to know during neonatal/infant spinal anesthesia
administration when the subarachnoid space is accessed from L4-
5 or L5-S1 space compared to L2-3, L3-4 space in adults.
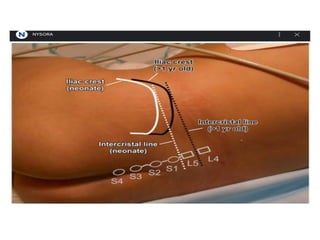
• The intercristal line serves as the landmark to identify the lumbar
vertebral level. This corresponds to L3-L4 in adults, while it
corresponds to L4-L5 in neonates.
9.
• The spinehas a single curve at birth.
• Cervical and lumbar lordosis develop as the infants achieve
milestones of head support and sitting. Adult configuration is
usually achieved by 1 year.
• Bones, including vertebrae, are not completely ossified at birth.
They are cartilaginous and offer little resistance to needle
advancement.
• Needles passed through non-ossified bones can potentially injure
the ossification nuclei.
10.
• The duralsac may extend down to S3-S4 in neonates and infants,
compared to S1 in adults. Because of this, caution has to be
exercised during the caudal block to prevent inadvertent dural
puncture.
• The sacral hiatus is covered by the sacrococcygeal ligament. This
space is wide open for infants, toddlers, and smaller children,
allowing easy access into the epidural space.
• Ossification and eventual closure of the hiatus, as well as the
changing axis of the coccyx, make the caudal block challenging in
older children and adults.
• Epidural fat is very fluid up to 8 years of age, aiding the extensive
spread of LA in children below this age.
• The spinous processes are more parallel and horizontal, allowing
easier midline access into the neuraxis.
11.
• The CSFvolume in a neonate is about 4 mL/kg, compared to the
adult volume of 2 mL/kg, and a greater proportion of this CSF
volume lives in the spinal subarachnoid space compared to adults.
• This is significant during neonatal/infant spinal anesthesia.
• The local anesthetic (LA) injected is immediately diluted by the
greater spinal CSF volume, necessitating a greater dose of local
anesthetic (up to 1 mg/kg of 0.5% bupivacaine) for the spinal block.
• The duration of action of the spinal anesthetic is also significantly
shorter compared to adults. Hence it is only suitable for brief
procedures.
12.
• Pharmacological differencesfrom adults result from different
anatomy at the neuronal level.
• Myelination is incomplete at birth; this can take up to 12 years to
complete.
• Due to this reason, a dilute local anesthetic will be able to provide a
denser block with a fast onset of action.
• However, the duration of the effect may be shorter than in adults
because of greater systemic absorption secondary to greater
cardiac output and decreased LA trapping in the immature sheath.
13.
• Amide localanesthetics are bound to plasma proteins, namely
alpha-acid glycoprotein and albumin.
• The free fraction of the LA contributes to systemic toxicity. Infants
have low levels of binding proteins, resulting in greater levels of
unbound LA. Adult levels are reached by 1 year of age.
• Cytochrome P450 enzymes necessary for the metabolism of
amide local anesthetics are immature in neonates.
• Ester local anesthetics are metabolized by plasma esterases.
Esterase activity is lower in neonates.
• All these enzyme activities gradually increase through the first year
of life.
15.
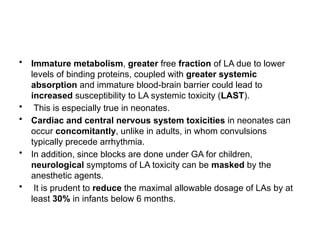
• Immature metabolism,greater free fraction of LA due to lower
levels of binding proteins, coupled with greater systemic
absorption and immature blood-brain barrier could lead to
increased susceptibility to LA systemic toxicity (LAST).
• This is especially true in neonates.
• Cardiac and central nervous system toxicities in neonates can
occur concomitantly, unlike in adults, in whom convulsions
typically precede arrhythmia.
• In addition, since blocks are done under GA for children,
neurological symptoms of LA toxicity can be masked by the
anesthetic agents.
• It is prudent to reduce the maximal allowable dosage of LAs by at
least 30% in infants below 6 months.
18.
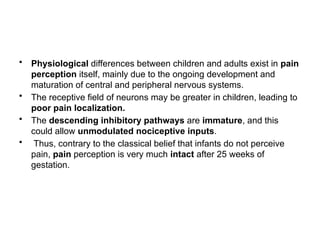
• Physiological differencesbetween children and adults exist in pain
perception itself, mainly due to the ongoing development and
maturation of central and peripheral nervous systems.
• The receptive field of neurons may be greater in children, leading to
poor pain localization.
• The descending inhibitory pathways are immature, and this
could allow unmodulated nociceptive inputs.
• Thus, contrary to the classical belief that infants do not perceive
pain, pain perception is very much intact after 25 weeks of
gestation.
19.
• The neurohormonalstress response to acute pain and risk of
chronic pain and behavioral problems secondary to acute pain
warrant meticulous and pre-emptive management of acute pain in
infants and children.
• Regional modalities play an important role in aiding this.
20.
Indications of CNBin pediatrics
• The epidural space includes thoracic, lumbar, sacral and
caudal routes and therefore provides
• analgesia and anaesthesia for thoracic, abdominal,
pelvic and lower limb procedures.
• Post operative analgesia
• as an adjuvant to GA
• for pre emptive analgesia
21.
Contraindications
• Contraindications topediatric regional anesthesia are similar to
those in adults.
• Absolute contraindications include patient or parent refusal and
local anesthetic allergy.
• True allergic reactions to LAs are relatively rare.
• Most of the “allergies” reported by the patient include reactions to
preservatives such as metabisulfite and methylparaben. Some are
symptoms of overdose toxicity.
22.
• Relative contraindicationsinclude
• infection at the needle insertion site,
• coagulopathy,
• sepsis,
• septicemia, and
• pre-existing neurologic deficit.
• Patients receiving anticoagulation medications can be managed
according to the American Society of Regional Anesthesia and Pain
Medicine (ASRA) guidelines.
23.
• Major vertebralanomalies can frequently be present in children
undergoing major urology, and lower limb orthopedic reconstruction
procedures.
• Therefore, caution is necessary when a neuraxial block is
considered for these children.
• In addition, pre-existing neurological deficits might be
considered a relative contraindication due to concern for the
progressive deficit.
• Children with these conditions should be assessed on a case-by-
case basis to evaluate the benefits and risks of performing the
block.
24.
REGIONAL ANESTHESIA: AWAKEOR
ASLEEP?
• Whether it is best for the patient to be awake or asleep during
regional anesthesia has been a controversial issue in adults, and
this debate once permeated the realm of pediatric regional
anesthesia practice.
• Placing a regional block in an awake child is difficult due to the
inability of the child to cooperate as well as the cognitive inability
of the child to relate to symptoms such as paresthesia or pain.
• Therefore, the child is best provided with a regional technique under
deep sedation or after the induction of general anesthesia;
25.
• However, thereare two scenarios in which awake regional
techniques are used in children.
• First, it was thought that by avoiding general anesthesia in
premature infants undergoing minor surgery, the incidence of
postoperative apnea could be reduced.
• This is probably less of an issue now that premature neonatal
lungs are better protected and with the availability of newer
inhalational agents that provide a more rapid emergence.
26.
• Second, themore mature child may be considered suitable for an
awake regional technique when undergoing a minor surgery.
• For older patients, it is essential to prepare the child and parents or
caregivers for the whole operating room visit, not just the insertion of
the block.
• The block insertion can be made more comfortable by applying a
topical anesthetic cream (EMLA has the best penetration) over the
proposed injection site.
• During the operating room visit, the child should be sup-ported and
distracted by a nurse or play specialist.
• The child may also find the use of a DVD or MP3 player a useful
distraction.
• It may be necessary to use nitrous oxide (Entonox) or anxiolytic
doses of propofol or remifentanil to ease proceedings.
27.
PERIOPERATIVE CNB
MANAGEMENT
• Somesimple rules need to be followed when performing any
regional anesthetic technique in children.
• A skilled assistant should be present at all times, and this
individual should understand the basic principles of regional
anesthesia, in particular the need to aspirate regularly prior to
injection, the need to warn the anesthesiologist about injection
resistance.
• Further, the assistant should be able to make basic adjustments to
the peripheral nerve stimulator (PNS) and US machines.
28.
• The childshould have a secure airway, intravenous access, and
full monitoring prior to commencing the block.
• As part of the World Health Organization (WHO) Surgical Safety
Checklist, consent and side of surgery are checked, and just
before block insertion, the site should again be confirmed with the
anesthesiologist’s assistant.
• The child, US machine (when used), equipment, and
anesthesiologist should be positioned ergonomically.
• Strict asepsis should be followed especially in catheter placement
procedures.
29.
Ultrasound in paediatric
anaesthesia
•Since it was first described by Ludwig in the 1940s, ultrasound has
become more portable and readily available, with enhanced image
quality.
• It can be used as an adjunct for regional anaesthesia (RA),
vascular access, airway management, bedside cardiac,
pulmonary and abdominal imaging, point-of-care ultrasound for
quick diagnostic purposes and intracranial pressure monitoring.
• The use of USG can improve success of procedures, enhance
safety and efficacy in daily clinical practice and assist with
therapeutic and diagnostic interventions.
30.
• A correctlydeposited volume of local anaesthetic (LA) may allow a
relatively opioid free general anaesthetic, with added advantages
of reducing postoperative nausea and vomiting, preventing
respiratory depression, enabling earlier mobilization, and
discharge home.
• Secondly, in children the anatomical structures of interest (i.e.
nerves and vessels) are more closely related, with lesser margins
of error using a landmark technique compared with adults.
• Ultrasound can also help to improve the precision of the block, as
the volumes that can be safely used are more tightly weight
restricted in children, and the safe practice of dissecting the tissue
planes with saline (‘hydro dissection’) before injecting the LA may
be limited in its scope for fear of dilution of the LA.
31.
Basics of ultrasound
•US describes sound waves with a frequency greater than 20 kHz.
• The US transducer uses the reverse piezoelectric effect to
generate US waves. These sound waves travel through tissues, all
with differing physical properties.
• A proportion of waves will be transmitted and some reflected back
to the US transducer, the piezoelectric effect converts this
mechanical energy to electrical energy and this produces the
image seen on the monitor.
32.
• Tissues thatallow the US beam to pass easily, e.g. fluid and
blood, appear dark (termed hypoechoic) whilst
• tissues that allow less beam to pass (reflect more sound waves),
e.g. fat and fascia, appear brighter on the US image (termed
hyperechoic).
• Bone reflects most of the sound, so is seen as having a thin
hyperechoic edge with a loss of sound transmission behind, which
appears black (anechoic) on the image.
33.
• The basicprinciples of image production are combined to create a
number of modes on a modern US machine.
• The most commonly used functions in anaesthesia are the B-mode,
the M-mode and colour-Doppler.
• B(brightness)-mode, where the brightness of each on-screen pixel
represents the magnitude of the signal reflected back to the
transducer, is used to scan in real time as the main mode on the
machine.
• M(motion)-mode examines the movement of structures along a
single axis and can be used to evaluate the motion of the heart
wall, valve, chest wall and haemodynamic status.
• Doppler mode is used to detect frequency shifts, formed by sound
reflections from a moving target, i.e. by utilising the Doppler effect.
34.
• The frequencyof the sound wave produced determines the smallest
object that can be visualised.
• Higher frequencies resolve smaller objects but do so at the
expense of depth of penetration.
• Common transducers used in paediatrics include
• linear high-frequency transducers with a large footprint, which
are useful for nerve blocks and neck and airway imaging,
• curvilinear multifrequency transducers for abdominal imaging,
• linear hockey stick high-frequency transducers with a small
footprint, useful for regional nerve blocks and vascular access in
smaller contact areas, and
• wideband-phased array transducers for cardiac imaging.
35.
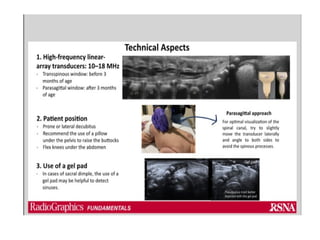
• Transducers inthe range of 10–15 MHz provide high spatial
resolution but limited depth penetration of waves, whereas
• lower frequency transducers (2–5 MHz) result in poorer image
resolution but offer deeper tissue penetration.
• In paediatrics, frequencies above 10 MHz would most often be
suitable.
• In children under 15 kg, a 25-mm transducer is usually suitable but
for children greater than 15 kg, a 50 mm transducer may be more
appropriate.
37.
• There aredifferent techniques for needle visualisation: in-plane
versus out-of-plane technique.
• In an in-plane approach, the needle is placed in the plane of the
US beam and therefore the entire shaft and needle tip can be seen.
• In an out-of-plane approach, the needle is placed perpendicular to
the transducer so a cross-section of the needle can be seen as a
dot on the image.
38.
USG GUIDED CNBs
•Technically, central neuraxial blocks in pediatrics have various
approaches.
• These blocks can be given as single shot or as continuous
techniques depending on the nature and severity of the surgical
procedure. These are
• Caudal epidural
• Lumbar epidural
• Thoracic epidural
• Spinal anaesthesia
39.
• US canidentify anatomical landmarks and the depth of the
epidural space.
• It also allows for needle visualisation and epidural catheter
advancement within the epidural space in neonates and infants.
• The ability of US to produce an image is impeded by bone, and
therefore, with increasing age and increased ossification, less of the
spinal column contents can be observed.
• Because of this fact, imaging of the spine in neonates can be done
with the transducer in the midline longitudinal position; however, in
infants and older age groups, a paramedian longitudinal approach is
used to obtain a view through the interlaminar space.
40.
• Paramedian longitudinaland the intervertebral axial planes
provide the best view of the spinal anatomy but the ultrasound
window size decreases with increasing age due to ossification.
• In addition, US may determine any structural abnormalities of the
spine that may contraindicate epidural blockade.
43.
Pediatric spinal anaesthesia
•Spinal anesthesia is perhaps one of the oldest and most studied
modalities for providing pain relief in patients undergoing surgery.
• J. Leonard Corning is credited with administering the first spinal
anesthetic in 1885, and his experience was subsequently published
in a medical journal.
• Although the use of intrathecal anesthesia administration in children
was described in the early twentieth century, this technique was
seldom used in the pediatric population until Melman reported a
series of high-risk infants who underwent successful surgery under
spinal anesthesia.
• Reports of apnea following general anesthesia in preterm infants
appeared in the literature in the early 1980s, and a series from
Abajian et al. offered practitioners an impetus to offer an alternative
technique with reportedly fewer complications than general
anesthesia.
44.
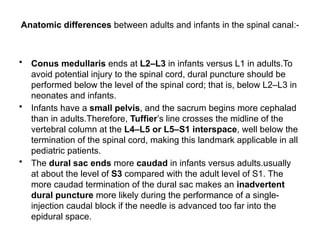
Anatomic differences betweenadults and infants in the spinal canal:-
• Conus medullaris ends at L2–L3 in infants versus L1 in adults.To
avoid potential injury to the spinal cord, dural puncture should be
performed below the level of the spinal cord; that is, below L2–L3 in
neonates and infants.
• Infants have a small pelvis, and the sacrum begins more cephalad
than in adults.Therefore, Tuffier’s line crosses the midline of the
vertebral column at the L4–L5 or L5–S1 interspace, well below the
termination of the spinal cord, making this landmark applicable in all
pediatric patients.
• The dural sac ends more caudad in infants versus adults.usually
at about the level of S3 compared with the adult level of S1. The
more caudad termination of the dural sac makes an inadvertent
dural puncture more likely during the performance of a single-
injection caudal block if the needle is advanced too far into the
epidural space.
45.
• CSF volumeis higher on a milliliter-per-kilogram basis in infants
and neonates (4 mL/kg) compared with adults (2 mL/kg).
• In addition, CSF in infants is distributed relatively more in the spinal
canal than in the head, as opposed to the distribution in adults.
• This may, in part, account for the higher local anesthetic dose
requirements and shorter duration of action of spinal anesthesia in
infants.
• The high cardiac output characteristic of the pediatric population
shortens the duration of spinal blocks in children still further.
49.
LOCAL ANESTHETICS
• Bupivacaine0.5%, 0.5–1 mg/kg, is generally used for spinal
anesthesia in children weighing less than 10 kg.
• A dose toward the higher end of the range is preferred for smaller
children; the risk of total spinal anesthesia is low as long as the
procedure is carried out diligently
• A hyperbaric bupivacaine solution with glucose 8% provides a block
of similar quality and duration than isobaric bupivacaine with
glucose 0.9%.
51.
• Adjuvants tolocal anesthetics in spinal blocks have also been
described.
• Clonidine in a dose of 1 mcg/kg added to bupivacaine (1 mg/kg)
used in spinal anesthesia for newborn infants has been shown to
prolong block duration to almost twice the duration of spinal
anesthesia without clonidine.
• However, the use of 2 mcg/kg of clonidine may cause a transient
decrease in blood pressure and greater postoperative sedation. It
may be advisable to use a dose of caffeine of 10 mg/kg
intravenously to prevent potential postoperative apnea, especially if
clonidine is used in the spinal anesthetic solution.
• Dexmedetomidine 1-2mcg/kg has also been suggested, however
less evidence is available for its use.
52.
• Adverse effectsfrom spinal anesthesia commonly seen in adults
are less common in children.
• These include hypotension, bradycardia, PDPH, and transient
radicular symptoms.
53.
Preparation
• Eutectic mixtureof local anesthetic (EMLA) cream or LMX (4%
lidocaine cream) may be applied to the site of insertion, although the
risk of methemoglobinemia must be taken into account in very
small premature infants.
• The operating room should be warmed before bringing the patient
into to the room. Warm blankets and radiant heating lamps help to
diminish heat loss in infants.
• With older children, the room should be quiet and, if possible,
surgical instruments covered to minimize patient anxiety.
• Standard monitoring devices (pulse oximeter, electrocardiogram,
and blood pressure cuff) should be applied before performing the
block.
• Older children may require supplemental sedation or light general
anesthesia prior to performing the block.
54.
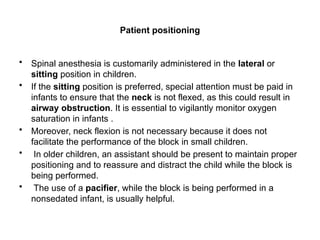
Patient positioning
• Spinalanesthesia is customarily administered in the lateral or
sitting position in children.
• If the sitting position is preferred, special attention must be paid in
infants to ensure that the neck is not flexed, as this could result in
airway obstruction. It is essential to vigilantly monitor oxygen
saturation in infants .
• Moreover, neck flexion is not necessary because it does not
facilitate the performance of the block in small children.
• In older children, an assistant should be present to maintain proper
positioning and to reassure and distract the child while the block is
being performed.
• The use of a pacifier, while the block is being performed in a
nonsedated infant, is usually helpful.
55.
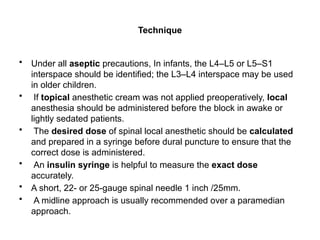
Technique
• Under allaseptic precautions, In infants, the L4–L5 or L5–S1
interspace should be identified; the L3–L4 interspace may be used
in older children.
• If topical anesthetic cream was not applied preoperatively, local
anesthesia should be administered before the block in awake or
lightly sedated patients.
• The desired dose of spinal local anesthetic should be calculated
and prepared in a syringe before dural puncture to ensure that the
correct dose is administered.
• An insulin syringe is helpful to measure the exact dose
accurately.
• A short, 22- or 25-gauge spinal needle 1 inch /25mm.
• A midline approach is usually recommended over a paramedian
approach.
56.
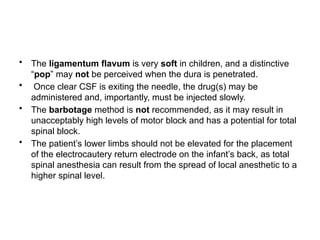
• The ligamentumflavum is very soft in children, and a distinctive
“pop” may not be perceived when the dura is penetrated.
• Once clear CSF is exiting the needle, the drug(s) may be
administered and, importantly, must be injected slowly.
• The barbotage method is not recommended, as it may result in
unacceptably high levels of motor block and has a potential for total
spinal block.
• The patient’s lower limbs should not be elevated for the placement
of the electrocautery return electrode on the infant’s back, as total
spinal anesthesia can result from the spread of local anesthetic to a
higher spinal level.
58.
Assessing the Block
•Assessing the level of block may prove difficult in infants and young
children, particularly in patients who have received sedation or in
those in whom the block is being performed under general
anesthesia.
• In infants, pinprick or response to cold stimuli (eg, an alcohol swab)
may be used, as well as observation of ventilation rate and pattern.
• In children over 2 years of age, the Bromage scale is used.
59.
EPIDURAL ANESTHESIA IN
CHILDREN
•Epidural analgesia is commonly used in addition to general
anesthesia and to manage postoperative pain.
• Effective postoperative pain relief from epidural analgesia has
numerous benefits including earlier ambulation, facilitating
weaning from ventilators, reducing time spent in a catabolic state,
and lowering circulating stress hormone levels.
• Precise placement of epidural needles for single-injection
techniques and catheters for continuous epidural anesthesia
ensures that the dermatomes involved in the surgical procedure are
selectively blocked, allowing for lower doses of local anesthetics to
be used and sparing unnecessary block in nondesired regions.
• The approach to the epidural space can be at the caudal, lumbar, or
thoracic level.
60.
• Ultrasound (US)assessment of the neuraxial structures is less
challenging in younger children because ossification is less
developed.
• In infants, the spinal cord fibers, the cerebrospinal fluid (CSF), and
the dura mater are easily identified using linear high-frequency US
probes.
• It has also been suggested that the epidural fat is less densely
packed in children than in adults. The loosely packed epidural fat
may facilitate the spread of local anesthetic and help achieve a
quicker block onset.
• It may also allow the unimpeded advancement of epidural catheters
from the caudal epidural space to the lumbar and thoracic levels.
However, the final placement of a catheter’s tip is best monitored
directly under US guidance or indirectly by identifying the injection of
local anesthetic.
61.
LOCAL ANESTHETICS FOREPIDURAL ANESTHESIA IN
CHILDREN
• Bupivacaine, ropivacaine, and levobupivacaine are the most
commonly used local anesthetics for neuraxial anesthesia in
children.
• Lidocaine is not often used because of its excessive motor block.
• As a general rule, high concentrations of local anesthetics, such as
0.5% bupivacaine or 0.5% ropivacaine, are seldom used in epidural
blocks in children.
• Instead, larger volumes of more dilute local anesthetic are more
commonly used to cover multiple dermatomes.
• Ideal Body weight is usually a better correlation than patient age
in predicting spread of local anesthetic after a caudal block.
62.
• A simplerule for a caudal single injection in children under 20 kg is
to use bupivacaine 0.125%–0.175% or ropiva-caine 0.2% and
give a bolus of one of the following:
• 0.5 ml/kg to achieve a sacral surgical level
• 1.0 ml/kg to achieve a high lumbar surgical level
• 1.25 ml/kg to achieve a low thoracic surgical level
• For continuous epidural infusion, bupivacaine 0.125% at a rate of
0.2 mg/kg/h for neonates and 0.4 mg/kg/h for older children is
often used.
• Ropivacaine 0.1% at a rate of 0.2 mg/kg/h for neonates and 0.4
mg/kg/h for older children for 48 hours has been shown to be an
effective and safe regimen.
64.
ADJUVANTS FOR EPIDURALANESTHESIA IN CHILDREN
• The most commonly used adjuvant to local anesthetics has been
epinephrine. Epinephrine in a concentration of 1:200,000 is used to
decrease the absorption rate of local anesthetic and has the added
benefit of serving as a possible marker for an inadvertent
intravascular injection.
• Epidural opioids may enhance the effect of local anesthetics and
prolong analgesia. 2 mcg/kg of fentanyl for single-injection
caudal anesthesia along with the standard local anesthetic solution
or addition of 1–2 mcg/mL fentanyl to 0.1% bupivacaine for
continuous epidural infusions has also been used with success in
children in a well-monitored inpatient setting.
• Epidural morphine when added to single-injection caudal epidural
blocks, it will enhance the level of block because of its rostral
dispersion (as morphine is a hydrophilic molecule). Doses of
caudal morphine vary from 30–90 mcg/kg depending on the type of
surgery.
65.
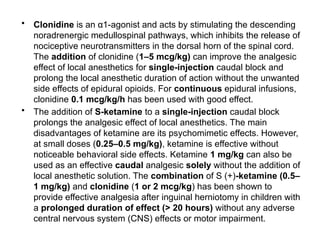
• Clonidine isan α1-agonist and acts by stimulating the descending
noradrenergic medullospinal pathways, which inhibits the release of
nociceptive neurotransmitters in the dorsal horn of the spinal cord.
The addition of clonidine (1–5 mcg/kg) can improve the analgesic
effect of local anesthetics for single-injection caudal block and
prolong the local anesthetic duration of action without the unwanted
side effects of epidural opioids. For continuous epidural infusions,
clonidine 0.1 mcg/kg/h has been used with good effect.
• The addition of S-ketamine to a single-injection caudal block
prolongs the analgesic effect of local anesthetics. The main
disadvantages of ketamine are its psychomimetic effects. However,
at small doses (0.25–0.5 mg/kg), ketamine is effective without
noticeable behavioral side effects. Ketamine 1 mg/kg can also be
used as an effective caudal analgesic solely without the addition of
local anesthetic solution. The combination of S (+)-ketamine (0.5–
1 mg/kg) and clonidine (1 or 2 mcg/kg) has been shown to
provide effective analgesia after inguinal herniotomy in children with
a prolonged duration of effect (> 20 hours) without any adverse
central nervous system (CNS) effects or motor impairment.
66.
Complications associated withepidural
anaesthesia
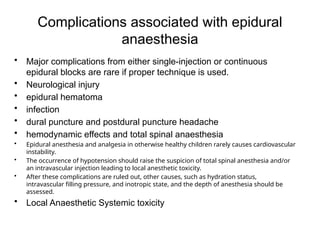
• Major complications from either single-injection or continuous
epidural blocks are rare if proper technique is used.
• Neurological injury
• epidural hematoma
• infection
• dural puncture and postdural puncture headache
• hemodynamic effects and total spinal anaesthesia
• Epidural anesthesia and analgesia in otherwise healthy children rarely causes cardiovascular
instability.
• The occurrence of hypotension should raise the suspicion of total spinal anesthesia and/or
an intravascular injection leading to local anesthetic toxicity.
• After these complications are ruled out, other causes, such as hydration status,
intravascular filling pressure, and inotropic state, and the depth of anesthesia should be
assessed.
• Local Anaesthetic Systemic toxicity
67.
Techniques of epiduralplacement
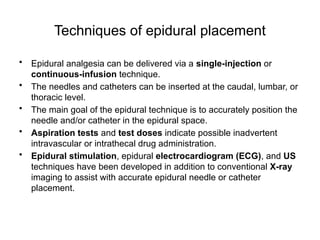
• Epidural analgesia can be delivered via a single-injection or
continuous-infusion technique.
• The needles and catheters can be inserted at the caudal, lumbar, or
thoracic level.
• The main goal of the epidural technique is to accurately position the
needle and/or catheter in the epidural space.
• Aspiration tests and test doses indicate possible inadvertent
intravascular or intrathecal drug administration.
• Epidural stimulation, epidural electrocardiogram (ECG), and US
techniques have been developed in addition to conventional X-ray
imaging to assist with accurate epidural needle or catheter
placement.
70.
Epidural Approaches
• Themost common types of epidural analgesia are
• caudal analgesia (which constitutes the most commonly used
regional technique in children),
• lumbar epidural analgesia, and
• thoracic epidural analgesia.
71.
CAUDAL EPIDURAL
• Thisis a simple and safe technique which fits most of the surgeries
below the umbilicus. Analgesic level above the umbilicus can also
be achieved.
• The five sacral vertebrae form the convex dorsal roof of the
space. Floor is formed by the base of sacrum.
• Anatomically the space is approached via the sacral hiatus, which
is formed by the sacral cornua on either side. The sacrococcygeal
membrane covers the sacral hiatus.
• The sacral nerves, filum terminale, venous plexus and fat are
contained in this enclosed space. It is imperative to note that dura
and the spinal cord reach lower levels in the spinal canal in infants
(spinal cord L3 at birth, L1/L2 at 1 year and dura S4 at birth, S2 at 1
year). In small infants, the end of the dural sac can be at a distance
of only a few millimetres from the puncture site.
• Recent applications of ultrasound make the anaesthesiologist
revisit anatomy.
72.
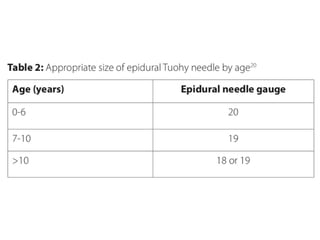
Caudal Epidural Analgesia:Single-Injection Technique
• Choice of Needle for Caudal Analgesia:
• The size or type of needle does not appear to affect the rate of
success or the incidence of complications of caudal block.
• Short-bevel Tuohy or Crawford needles (5 cm in length) with
stylets offer a better tactile sensation when the sacrococcygeal
ligament is punctured.
• For children aged 1 year or older, a 22-gauge needle is used;
• for children younger than 1 year of age, a 25-gauge needle may
be used.
• The use of a styletted needle may reduce the risk of introducing a
dermal plug into the caudal space, although an epidermal cell graft
tumor in the epidural space has yet to be reported.
73.
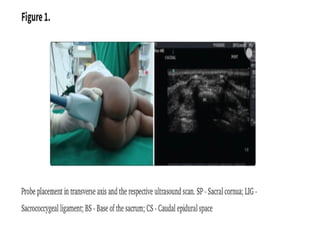
• Caudal epiduralsonoanatomy
• The caudal space can be visualised in two views, transverse and
longitudinal.
• Transverse scan:-
• The position of the probe is as shown in Figure 1.
• The scan shows two hyperechoic sacral cornua and dark acoustic
shadows posterior to each of them. The hyperechoic fibrous
structure intervening between them is the sacrococcygeal
membrane or ligament. Posterior to the sacrococcygeal membrane
is the base of the sacrum [Figure 1].
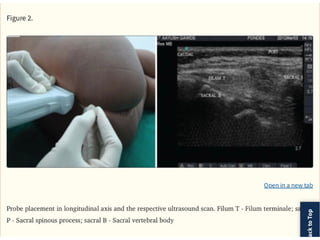
• Longitudinal scan
• Position of the probe is as shown in Figure 2. The sacral vertebrae,
the filum terminale and termination of the dural sac (conus
medullaris) can be identified in the longitudinal axis [Figure 2]. The
filum terminale is a cordlike hyperechoic structure and is
surrounded by hyperechoic nerve roots of the cauda equina. It is
difficult to differentiate filum terminale from the nerve roots due to
their identical appearance (both appear like hyperechoic strands).
76.
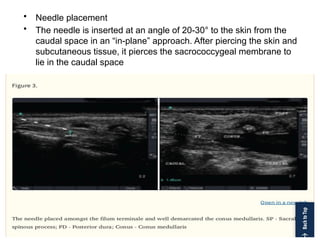
• Needle placement
•The needle is inserted at an angle of 20-30° to the skin from the
caudal space in an “in-plane” approach. After piercing the skin and
subcutaneous tissue, it pierces the sacrococcygeal membrane to
lie in the caudal space
77.
• Local anaestheticinjection and its spread in the caudal space as
seen under ultrasound guidance
• The observation of real-time drug spread in the caudal epidural
space has unveiled a lot of facts pertaining to its cranial spread
• Posterior dural sag [Figure 4] as the drug displaces posterior dura
anteriorly while making its way in the cehaplic direction is taken as
a surrogate marker for correct drug placement.
78.
CONTINUOUS CAUDAL EPIDURALBLOCKS (CAUDO-
LUMBAR-THORACIC ANAESTHESIA)
• A single-shot caudal can be converted into a continuous
technique depending upon the invasiveness of the surgery.
• These catheters can be safety kept for 3-4 days in the
postoperative period.
• A catheter can be threaded up cranially through the sacral hiatus
via simple plastic cannula, Tuohy needles, or specifically designed
stimulating catheter sets with appropriate gauge needles (19 G,
Pjunk).
• This technique carries a smaller risk of dural puncture or spinal
cord trauma than a direct thoracic or lumbar epidural approach.
• Although malpositionings are known, they can be reduced by the
use of large bore catheters (18 G) and catheters with a stylet .
• The catheter tip position can be confirmed by
radiography,ultrasound,ECG tracing or electrostimulation.
79.
Issues with continuouscaudal technique
• Its proximity to anal region makes it prone to infections although
they are not very common.Subcutaneous tunnelling can decrease
colonisation as the catheter is tunnelled inside the subcutaneous
tissue
• Catheter leaks: In practice, we often observe a back leak of local
anaesthetic while injecting it through the caudal catheters. This can
be reduced by injecting the drug at a slow rate
• As mentioned earlier, the catheters need not always reach the site
that we expect them to by external measurements resulting in
inadequate analgesia.
80.
LUMBAR EPIDURAL
• Lumbarepidural can be practised as a single shot and continuous
technique.
• In children, since caudal epidural is technically much easier and
safer to practise for intra-abdominal minor surgeries, the risk benefit
ratio is advantageous for continuous technique for intra- and post-
operative analgesia for major surgeries.
• Again, the pursuit of regional techniques today is to be more and
more site specific. The catheters are introduced as close to the level
of incision as possible.
• Lesser the distance a catheter is expected to travel in the epidural
space, lesser is its chance to migrate, coil or take any unwanted
route.
82.
• Technique forlumbar epidural block:-
• Epidural space is identified by loss of resistance technique.
• Loss of resistance can be elicited with either air or saline. Although
air is readily available and cannot be confused for another
substance, and also may permit easier detection of a dural tap
compared to saline in children, loss of resistance is elicited by saline
instead of air.
• Many complications have been reported with the use of air such as
venous air embolism, nerve root compression, subcutaneous
emphysema, pneumocephalus, a greater incidence of incomplete
analgesia and a higher incidence of paresthesia
• Needle: 19 G with 21 G catheter and 18 G with 20 G catheters
Touhy (B Braun and Portex), stimulating epidural catheters (Pjunk)
available with 19 G stimulating Touhy needles and 21 G stimulating
catheters (Pjunk).
84.
THORACIC EPIDURAL
• Controversyexists concerning the safety of placing thoracic
epidurals under heavy sedation or general anesthesia, because
unconscious patients are unable to report symptoms that may warn
the anesthesiologist of potential neurologic complications
• Direct needle trauma to the spinal cord during epidural insertion is
rare but can cause devastating complications. For thoracic surgery,
the catheter should be introduced as close to the dermatomal level
of incision as is possible.
• The advancement of catheters from the lumbar and caudal epidural
spaces to the thoracic level is an alternative only in children upto 1
year of age.
• However, the advancement of catheters in the epidural space
becomes increasingly difficult with advancing age because of the
development of the lumbar curvature.
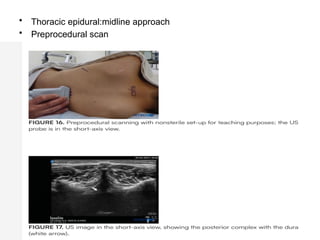
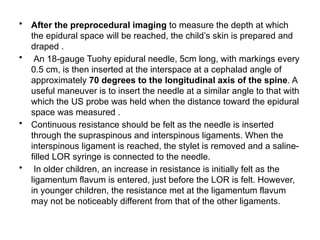
• After thepreprocedural imaging to measure the depth at which
the epidural space will be reached, the child’s skin is prepared and
draped .
• An 18-gauge Tuohy epidural needle, 5cm long, with markings every
0.5 cm, is then inserted at the interspace at a cephalad angle of
approximately 70 degrees to the longitudinal axis of the spine. A
useful maneuver is to insert the needle at a similar angle to that with
which the US probe was held when the distance toward the epidural
space was measured .
• Continuous resistance should be felt as the needle is inserted
through the supraspinous and interspinous ligaments. When the
interspinous ligament is reached, the stylet is removed and a saline-
filled LOR syringe is connected to the needle.
• In older children, an increase in resistance is initially felt as the
ligamentum flavum is entered, just before the LOR is felt. However,
in younger children, the resistance met at the ligamentum flavum
may not be noticeably different from that of the other ligaments.
87.
POSTOPERATIVE EPIDURAL
INFUSION MANAGEMENT
•For postoperative analgesia, either bupivacaine 0.125% or
ropivacaine 0.1–0.2%, with or without fentanyl 1–2 mcg/mL, is
administered at the following rates:
• Age > 3 months: 0.20–0.35 mL/kg/h (< 0.4 mg/kg/h bupivacaine)
• Age < 3 months: 0.1–0.15 mL/kg/h (< 0.2 mg/kg/h bupivacaine)
88.
SUMMARY
• Paediatric regionalanaesthesia should be amongst the anaesthetic
techniques offered by any paediatric anaesthetist.
• The benefits conferred have been shown repeatedly to be superior
to opioid analgesia and outweigh the risks, historically misconceived
to be high, but which are actually, and reassuringly, low.
• Ancillary techniques to access safely the neuraxial space are
increasing both block safety and success.
• Moreover, the widespread availability of ultrasound is facilitating a
range of blocks remote to the neuraxis with acceptable efficacy and
safety.
• The small amount of time added to the induction sequence before
the patient is ready for surgery is insignificant compared with the
time saved at every other stage of perioperative care, and is entirely
justified by the postoperative benefits to patients, staff and carers.













![• Caudal epidural sonoanatomy
• The caudal space can be visualised in two views, transverse and
longitudinal.
• Transverse scan:-
• The position of the probe is as shown in Figure 1.
• The scan shows two hyperechoic sacral cornua and dark acoustic
shadows posterior to each of them. The hyperechoic fibrous
structure intervening between them is the sacrococcygeal
membrane or ligament. Posterior to the sacrococcygeal membrane
is the base of the sacrum [Figure 1].
• Longitudinal scan
• Position of the probe is as shown in Figure 2. The sacral vertebrae,
the filum terminale and termination of the dural sac (conus
medullaris) can be identified in the longitudinal axis [Figure 2]. The
filum terminale is a cordlike hyperechoic structure and is
surrounded by hyperechoic nerve roots of the cauda equina. It is
difficult to differentiate filum terminale from the nerve roots due to
their identical appearance (both appear like hyperechoic strands).](https://image.slidesharecdn.com/paediatriccnbruby-250526111808-64d985d7/85/paediatric-central-neuraxial-block-presentation-73-320.jpg)
![• Local anaesthetic injection and its spread in the caudal space as
seen under ultrasound guidance
• The observation of real-time drug spread in the caudal epidural
space has unveiled a lot of facts pertaining to its cranial spread
• Posterior dural sag [Figure 4] as the drug displaces posterior dura
anteriorly while making its way in the cehaplic direction is taken as
a surrogate marker for correct drug placement.](https://image.slidesharecdn.com/paediatriccnbruby-250526111808-64d985d7/85/paediatric-central-neuraxial-block-presentation-77-320.jpg)































![Pharmacology for pediatric anaesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacologyforpediatricanaesthesiaautosaved-200626150216-thumbnail.jpg?width=640&height=640&fit=bounds)








































