Downloaded 39 times



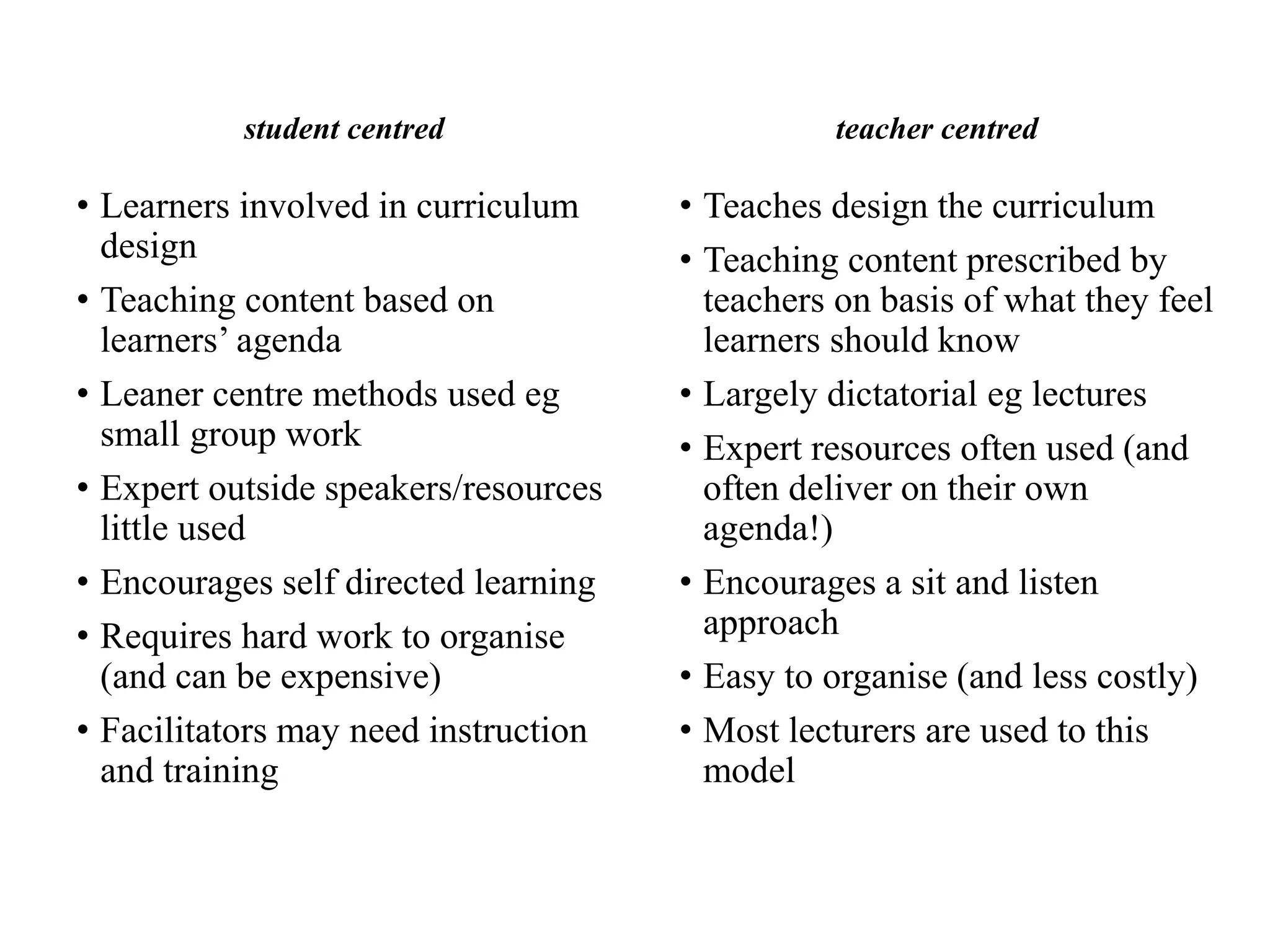




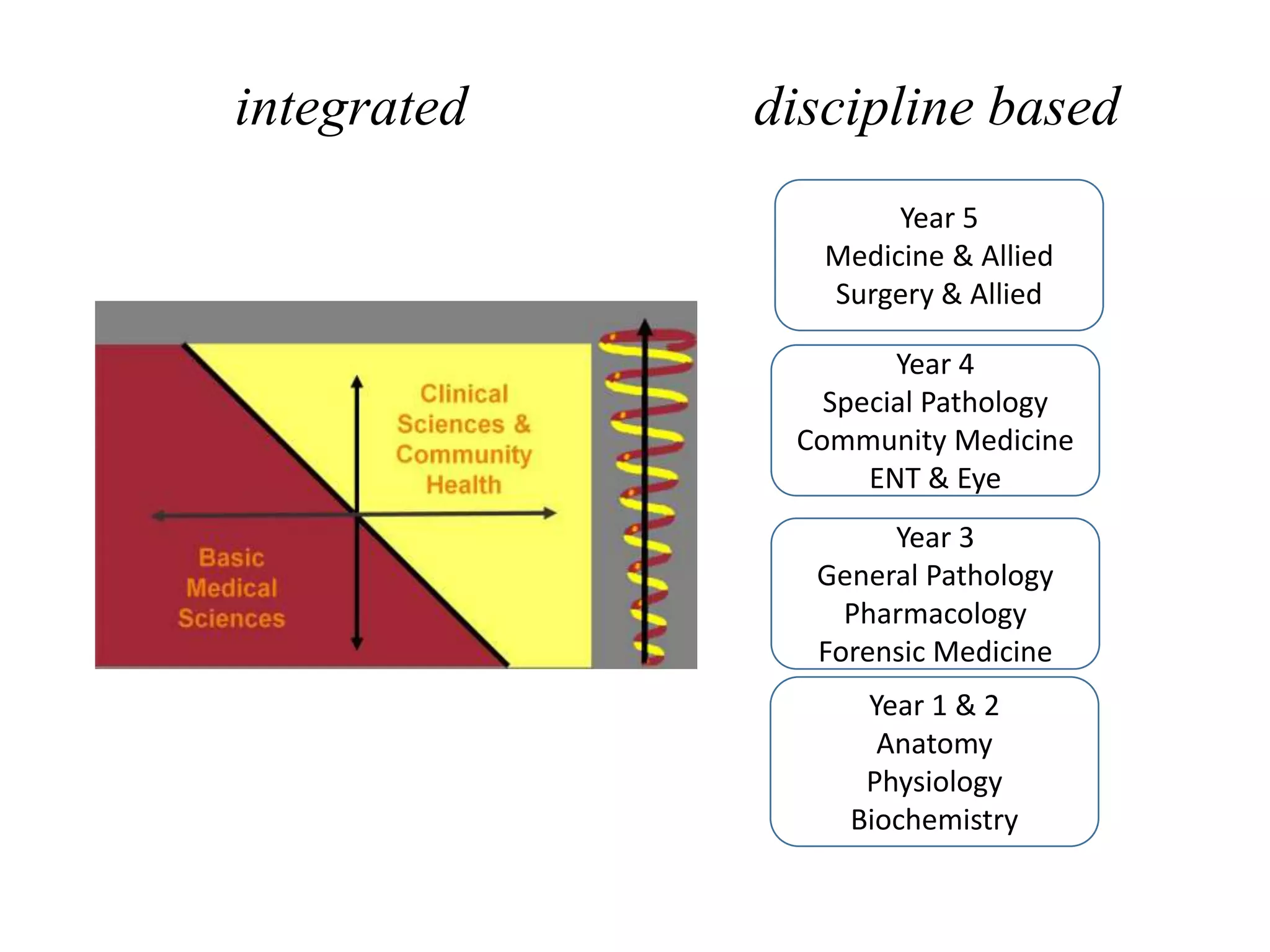








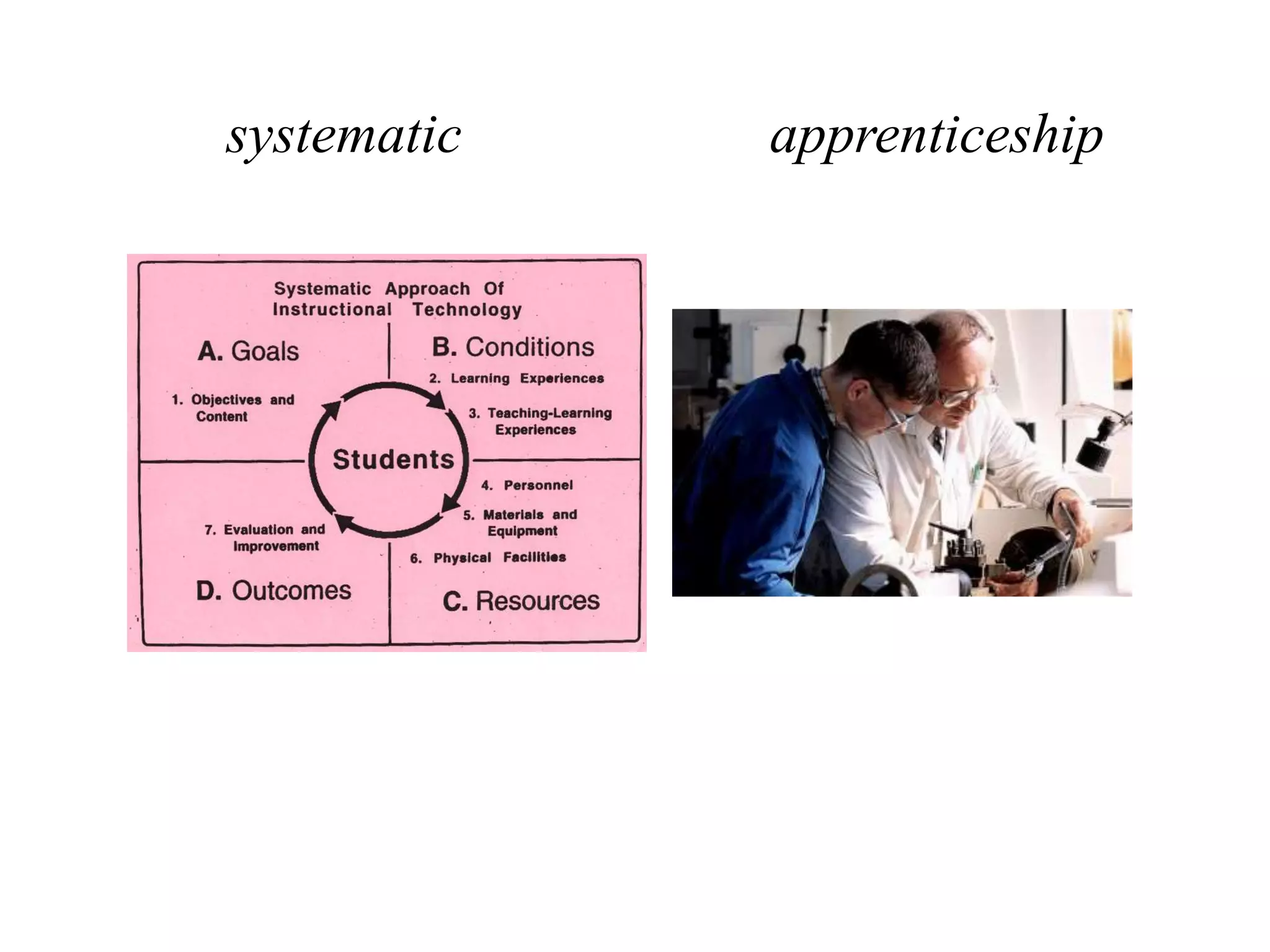
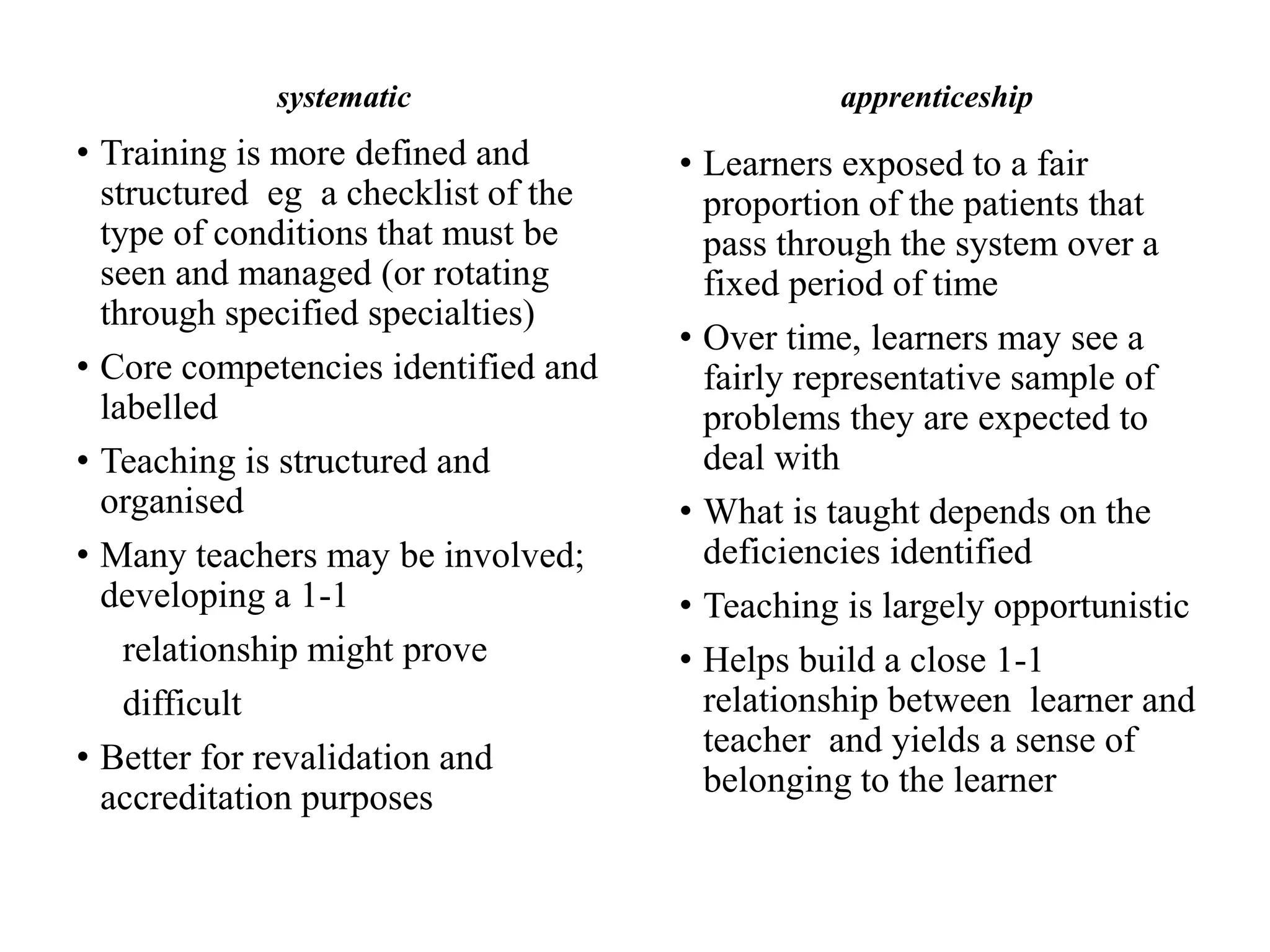


The document discusses various educational strategies in curriculum development using the SPICES model, emphasizing student-centered versus teacher-centered approaches, problem-based versus information gathering techniques, and community-based versus hospital-based learning. It highlights the benefits and drawbacks of each strategy, including their impact on learner motivation, knowledge retention, and the integration of disciplines. The document presents a structured overview of how to effectively design and implement curricula that cater to diverse learning needs while addressing specific community and educational goals.
























































![Mental health legislation altaf qadir [autosaved] usman ppt](https://cdn.slidesharecdn.com/ss_thumbnails/mentalhealthlegislationaltafqadirautosavedusmanppt-200323165733-thumbnail.jpg?width=640&height=640&fit=bounds)






























