Based on the limited information provided:
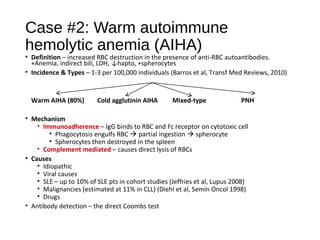
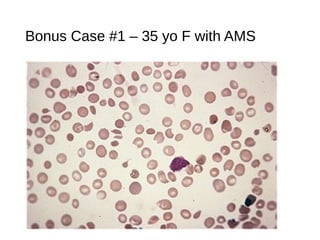
- Diagnosis: Thrombotic thrombocytopenic purpura (TTP)
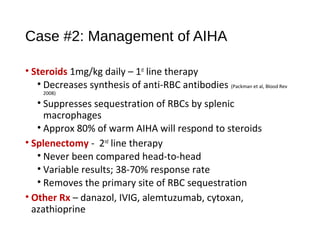
- Management: Plasma exchange to remove ADAMTS13 inhibitor
More information is needed to confirm the diagnosis and guide appropriate treatment. Some key questions include:
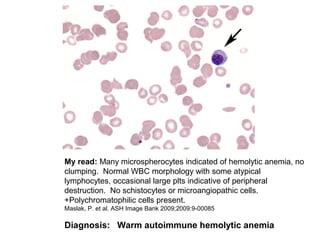
- Is there evidence of schistocytes on the peripheral smear?
- What is the patient's coagulation profile and haptoglobin level?
- Is ADAMTS13 activity level reduced?
- What is the patient's medical history and any potential triggers?
- Are there any neurologic deficits on exam beyond altered mental status?
Without confirming the presence of schistocytes and reduced ADAMTS13


























































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)





























