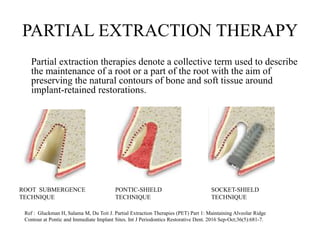
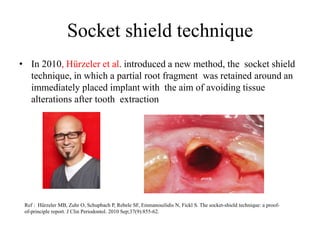
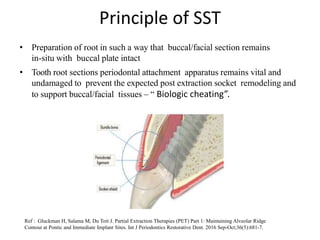
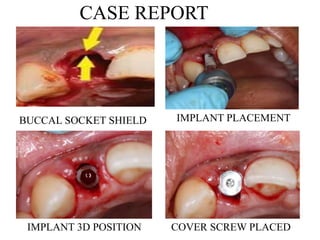
1. The socket shield technique involves retaining a portion of the root after extraction to preserve the buccal bone and soft tissue contours for an immediately placed implant.
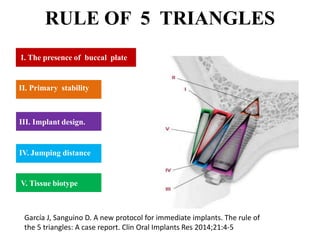
2. Key factors for success include primary stability of the implant, presence of the buccal plate, and thin soft tissue biotype.
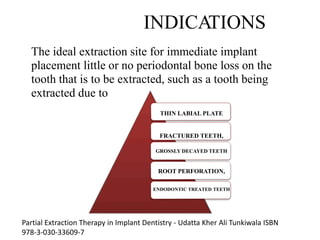
3. Advantages are optimal soft tissue esthetics, preservation of bone, and reduced treatment time. Indications are thin labial plates or fractured/decayed teeth.
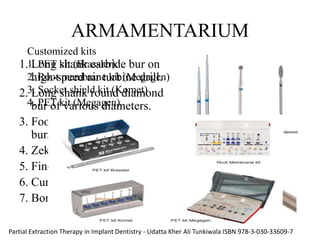
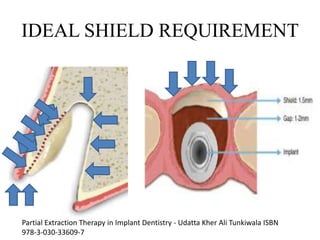
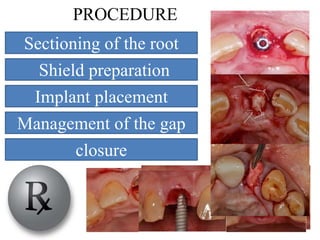
4. The procedure involves sectioning the root and preparing a buccal shield for the implant to be placed immediately adjacent to. Studies show bone formation between the shield and implant over time.


































![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)











































