Download to read offline


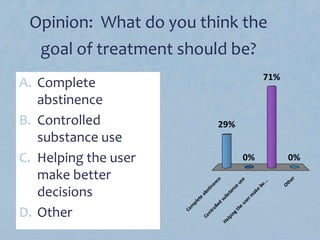
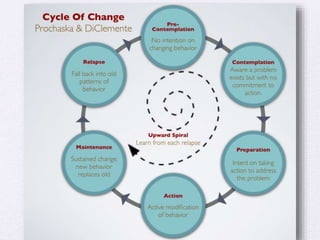
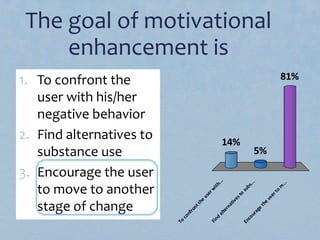

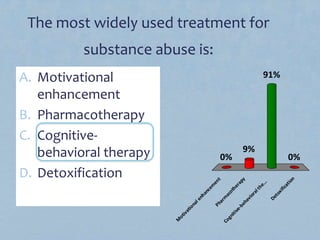
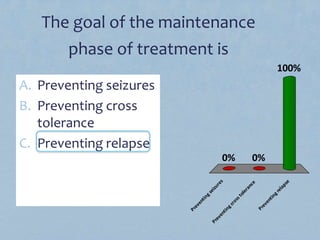

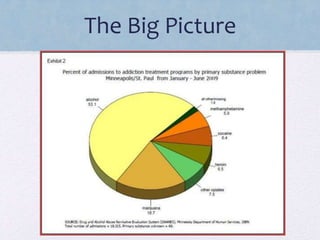


This document discusses substance abuse treatment. It covers various treatment programs like inpatient, outpatient, counseling, pharmacotherapies, and 12-step models. The key goals of treatment include defining treatment goals and helping users move through stages of change like pre-contemplation and contemplation. Treatment is most effective when the program matches the individual's needs. Relapse is common due to negative emotions, conflicts, and social pressures. Overall, treatment is beneficial by reducing drug use, criminal behavior, and health risks.









































































































