Download to read offline

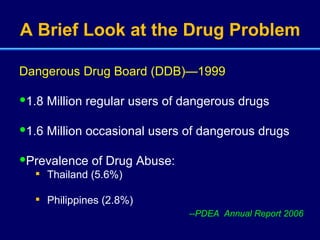
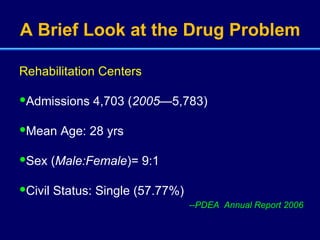
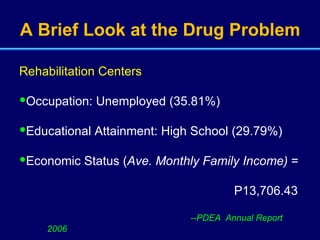
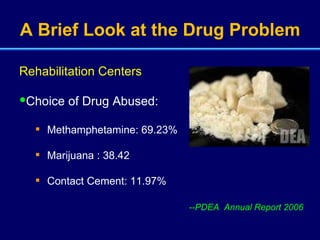
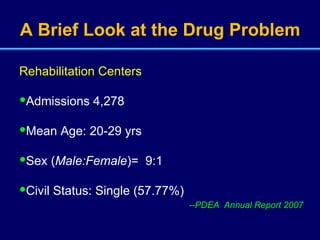













The document discusses the drug problem and treatment of drug dependence in the Philippines. It provides statistics on drug use and admissions to rehabilitation centers. It then covers the psychological dimensions of drug problems, reasons for drug use, treatment processes including discontinuation of substance use and behavioral modification, and prevention strategies.
















































![Energy%20drink[1]](https://cdn.slidesharecdn.com/ss_thumbnails/energy20drink1-100810063022-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























