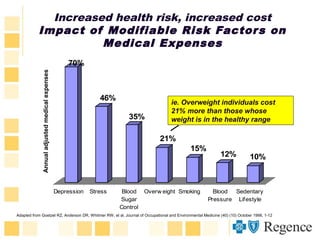
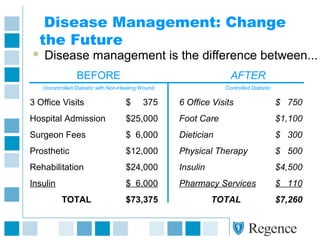
This document summarizes the key aspects of a health management program. It discusses how the program addresses various health risks and conditions across the care continuum from wellness to disease management. It provides data on common health risks and costs associated with them. The program utilizes nurses and health coaches to provide various services including wellness coaching, decision support, health coaching during pregnancy, case management, and disease management. It aims to help individuals better manage their health conditions and make improvements in clinical outcomes and costs through personalized support and education.








































![Alls Well Program Web[1]](https://cdn.slidesharecdn.com/ss_thumbnails/allswellprogramweb1-12893167748702-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Tempest Program[1]](https://cdn.slidesharecdn.com/ss_thumbnails/tempestprogram1-12893168208237-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![Wooden O Program[1]](https://cdn.slidesharecdn.com/ss_thumbnails/woodenoprogram1-12893168581327-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




















