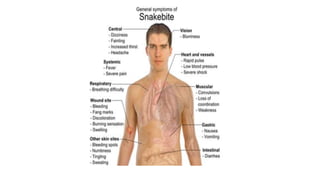
Snakes and scorpions can inject venom through bites or stings that is dangerous and sometimes fatal. There are over 50,000 deaths from snake bites worldwide each year. Venoms vary and can be neurotoxic, vasculotoxic, or myotoxic. Immediate medical help is needed for bites. Scorpion venom can also be neurotoxic or haemolytic, causing local or systemic effects like paralysis, cardiac issues, or death in severe cases. Treatment involves immobilization, antivenom, supportive care, and monitoring for complications.