Downloaded 120 times

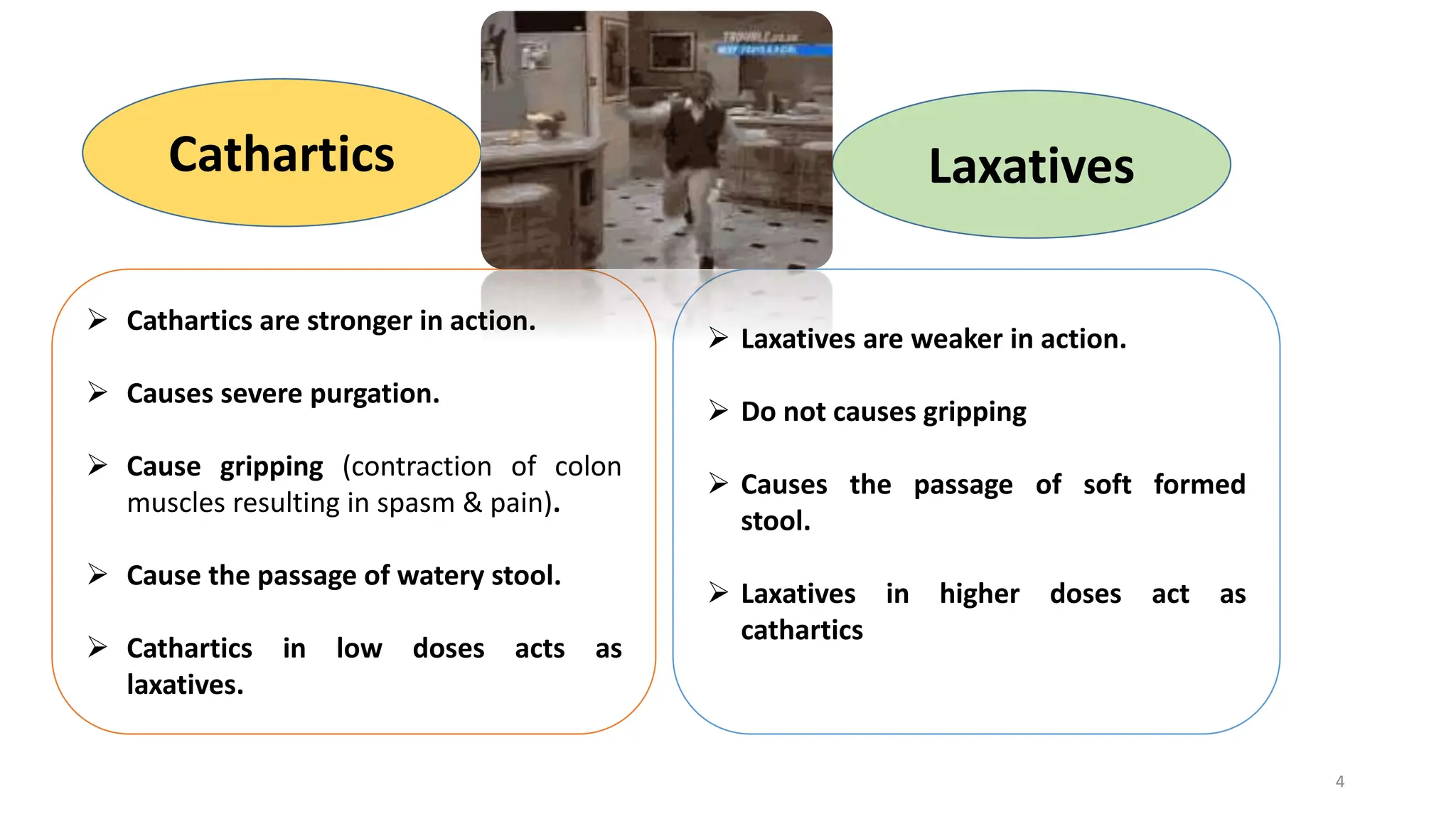
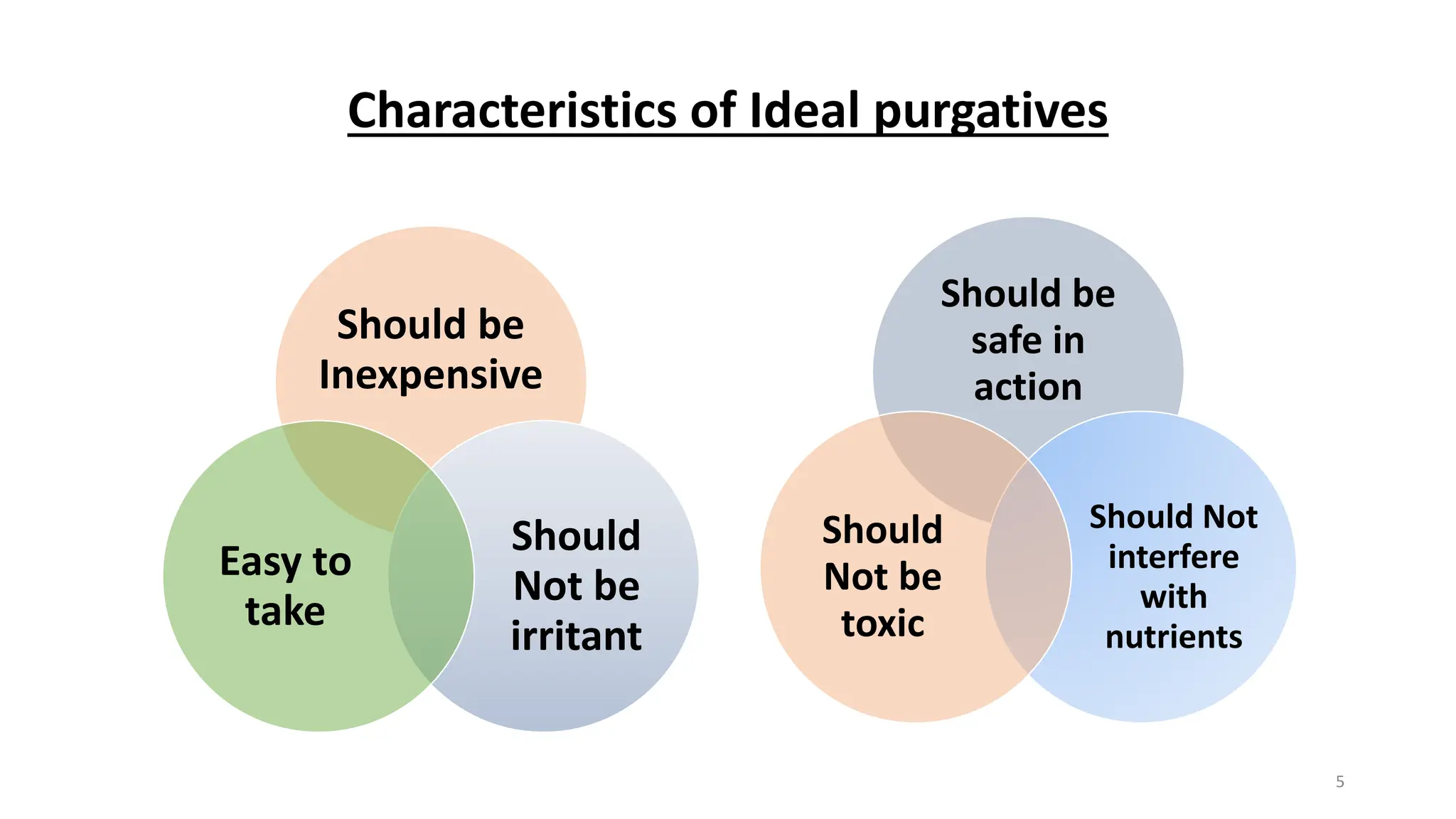



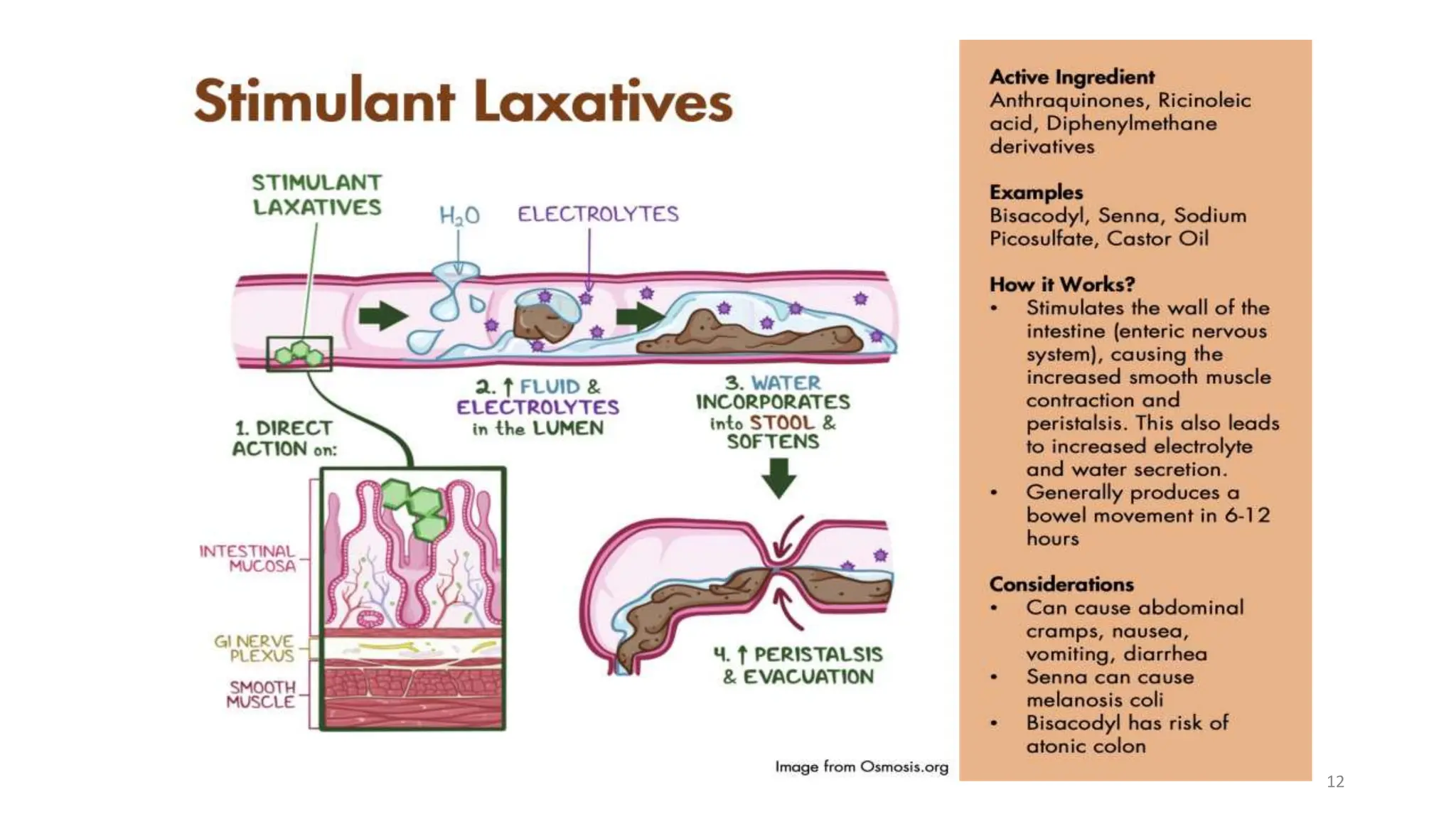




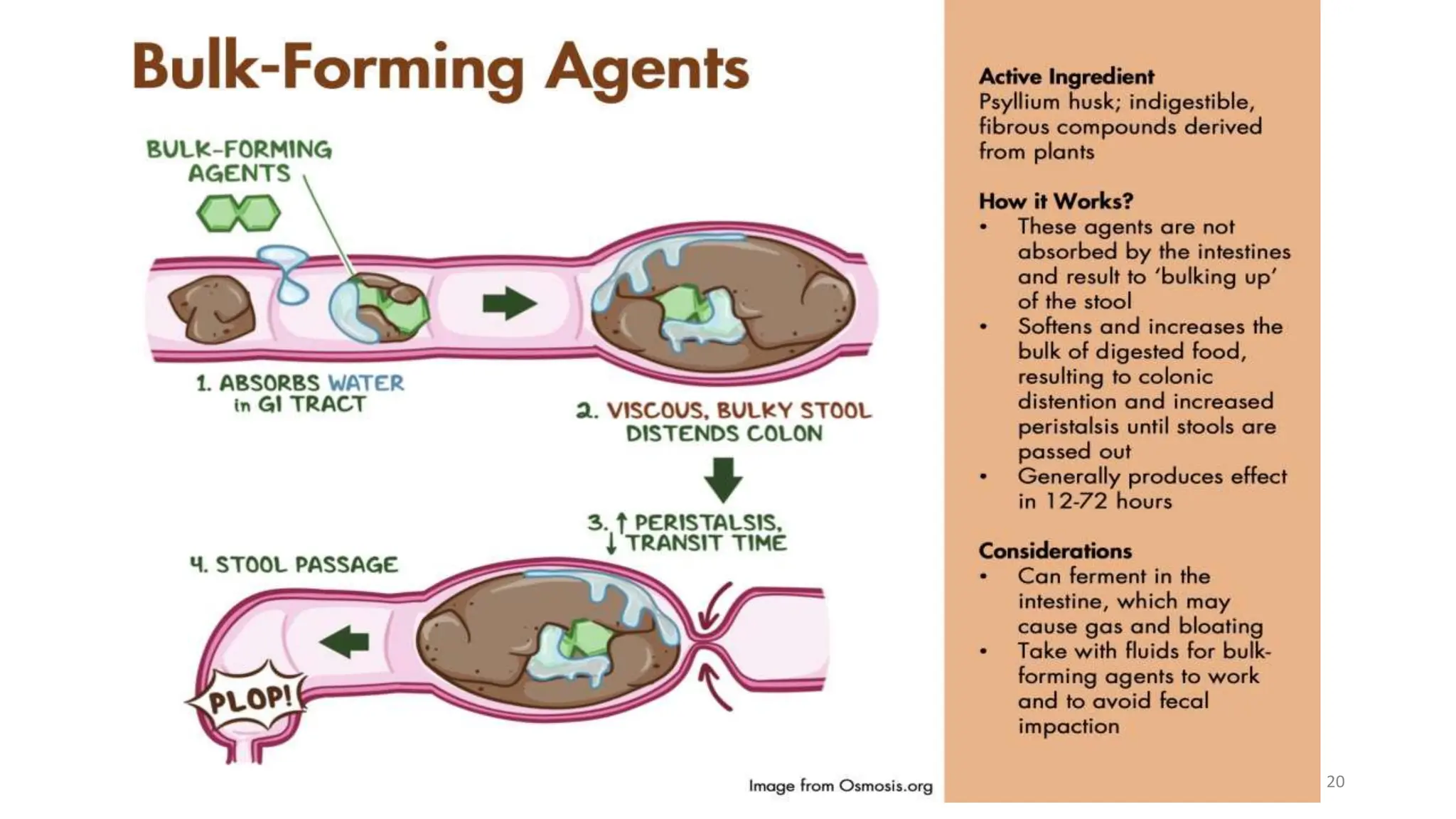


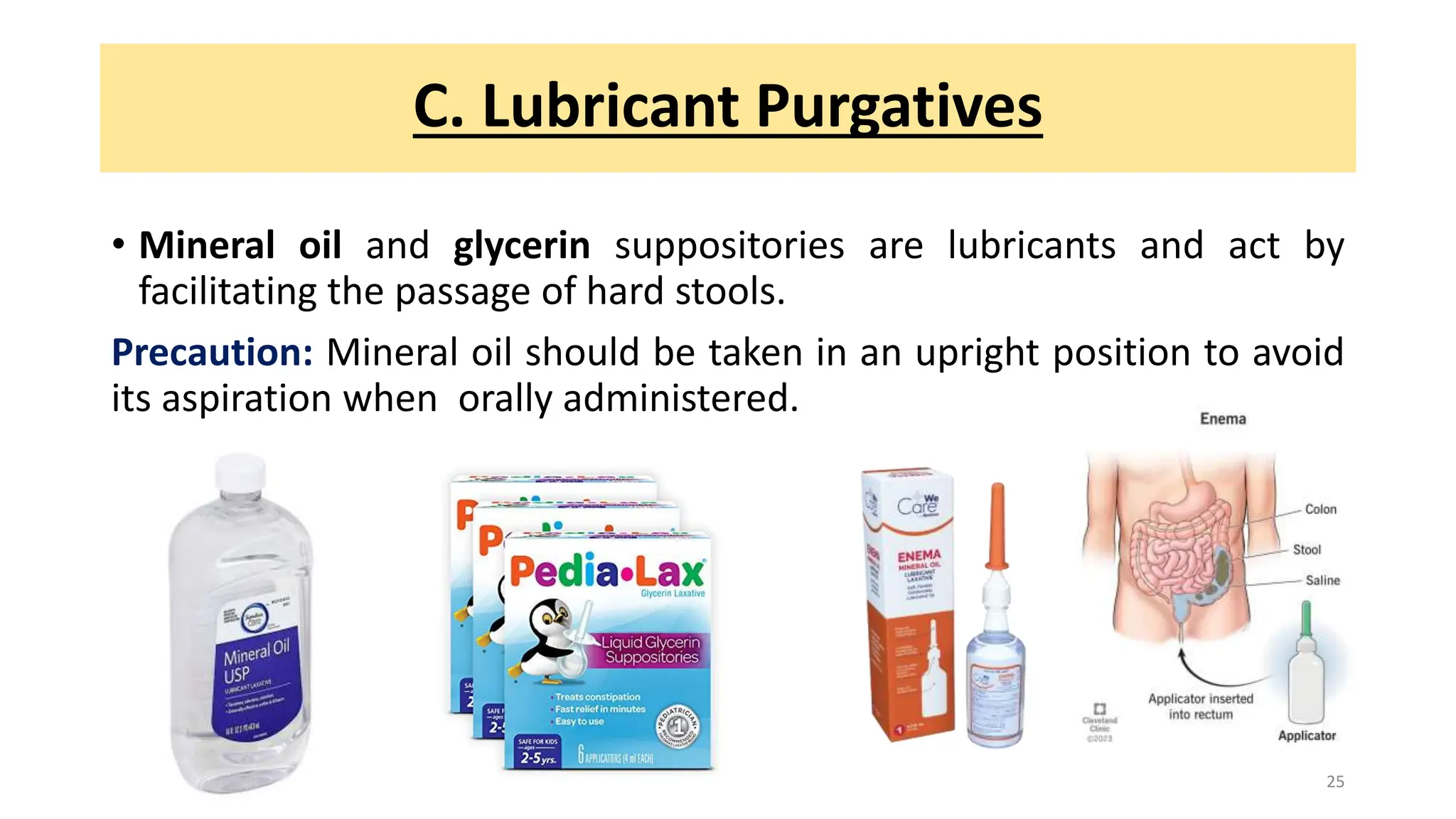
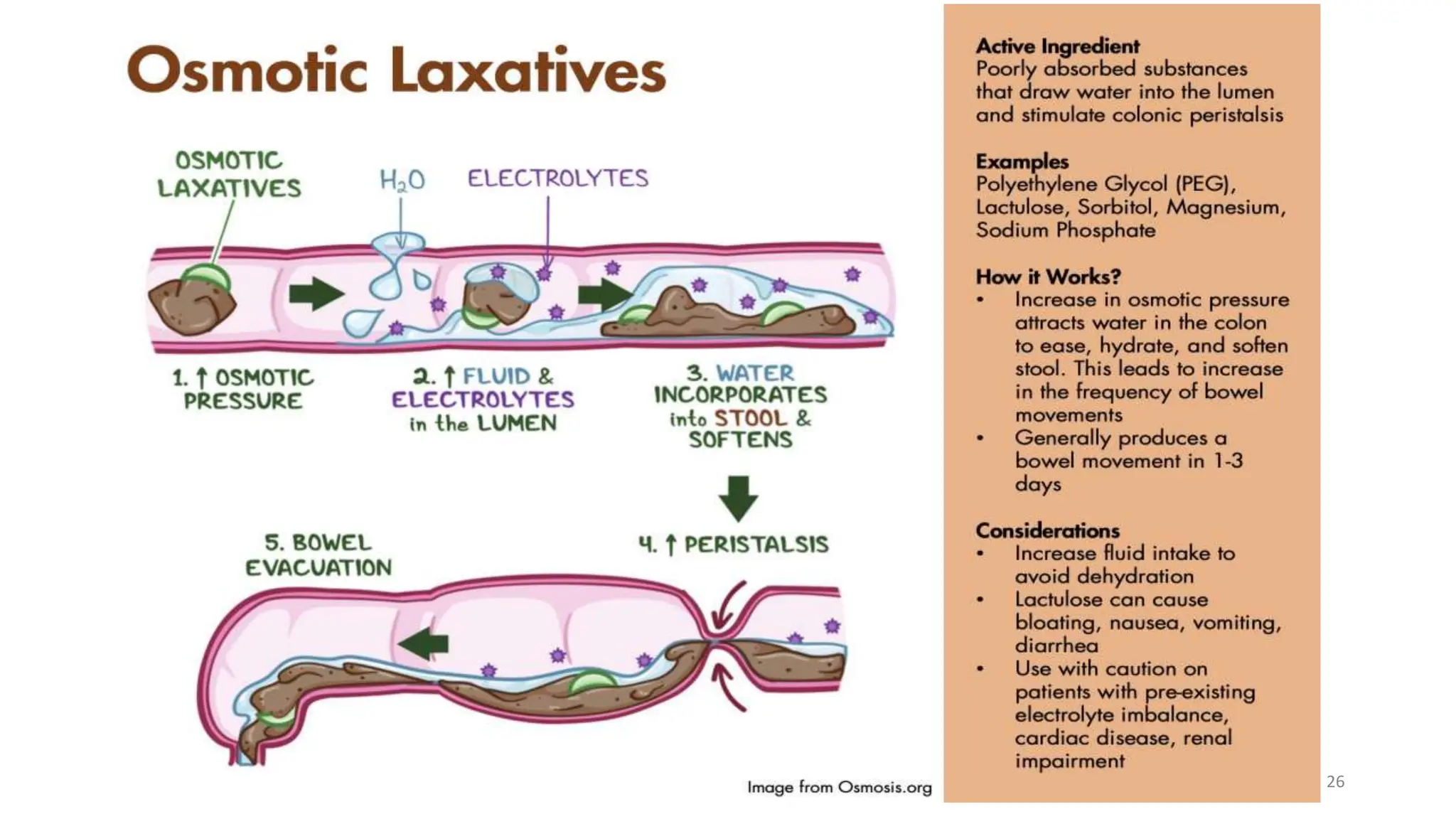



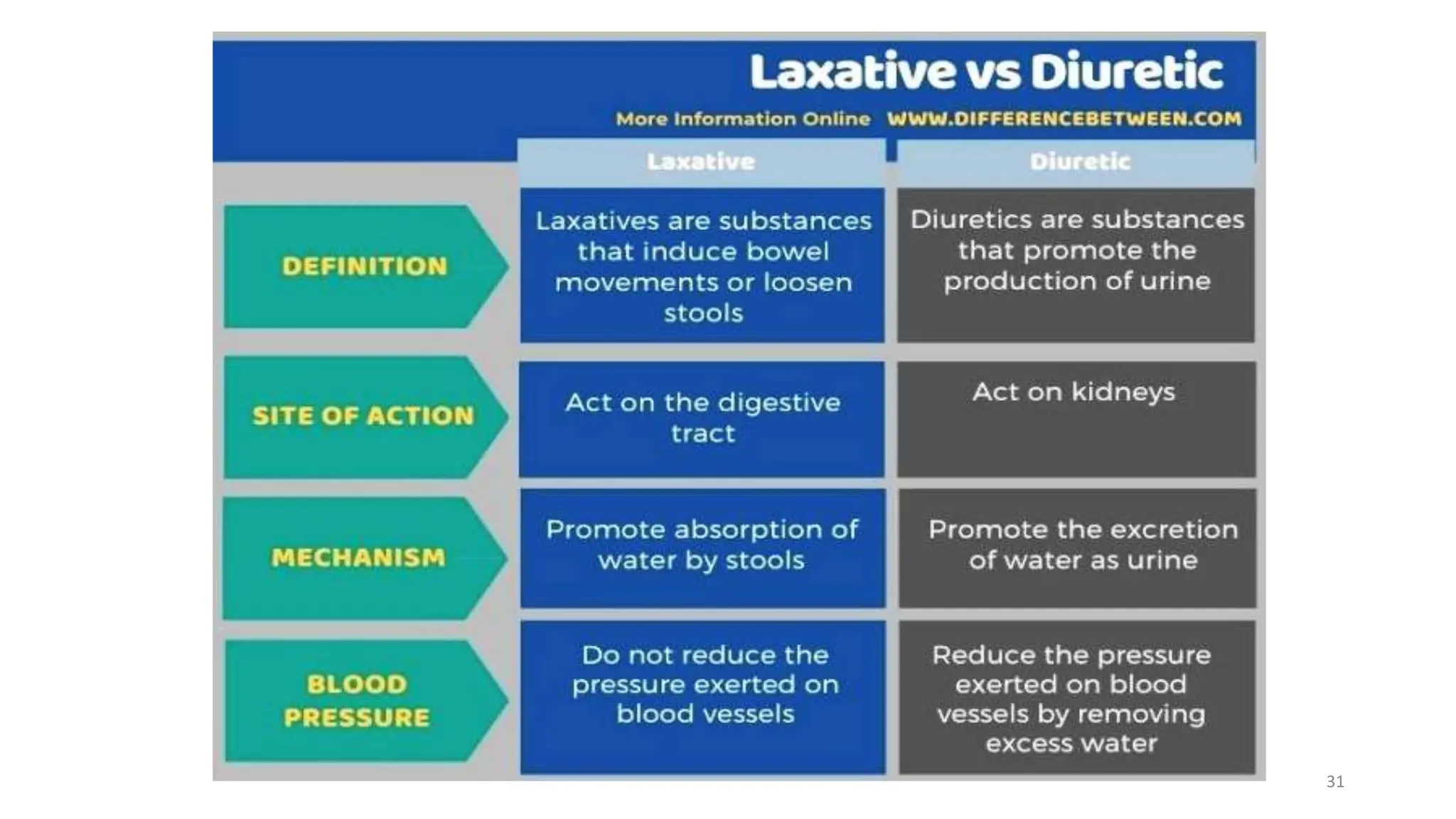


Purgatives and laxatives are drugs used to treat constipation by promoting bowel movements. They work through various mechanisms like increasing stool volume, stimulating intestinal contractions, or softening stool. Common types include bulk forming laxatives like psyllium husk, osmotic laxatives like lactulose, stimulant laxatives like senna and bisacodyl, and stool softeners. The ideal laxative is inexpensive, safe, and does not interfere with nutrient absorption while effectively treating constipation with minimal side effects.























































































