
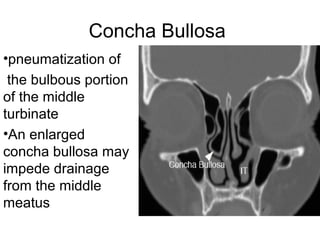

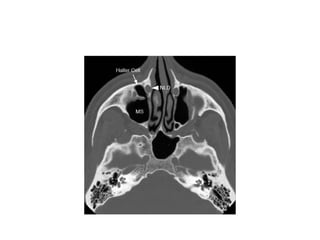
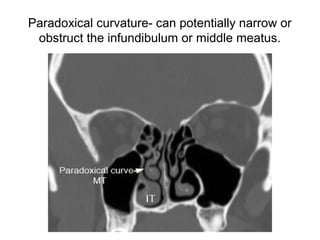




The document discusses the anatomy and variants of the paranasal sinuses relevant to functional endoscopic sinus surgery (FESS). It describes the four paired sinuses and their drainage pathways. Key anatomical structures for drainage include the osteomeatal complex and frontal recess. Common anatomic variants are described such as concha bullosa, Haller cells, and Onodi cells which can impact sinus drainage. Radiologists should evaluate pre-operative scans for variants that may obstruct drainage or pose surgical hazards. A systematic checklist is recommended to identify issues important for surgical planning.





























































































