Downloaded 16 times

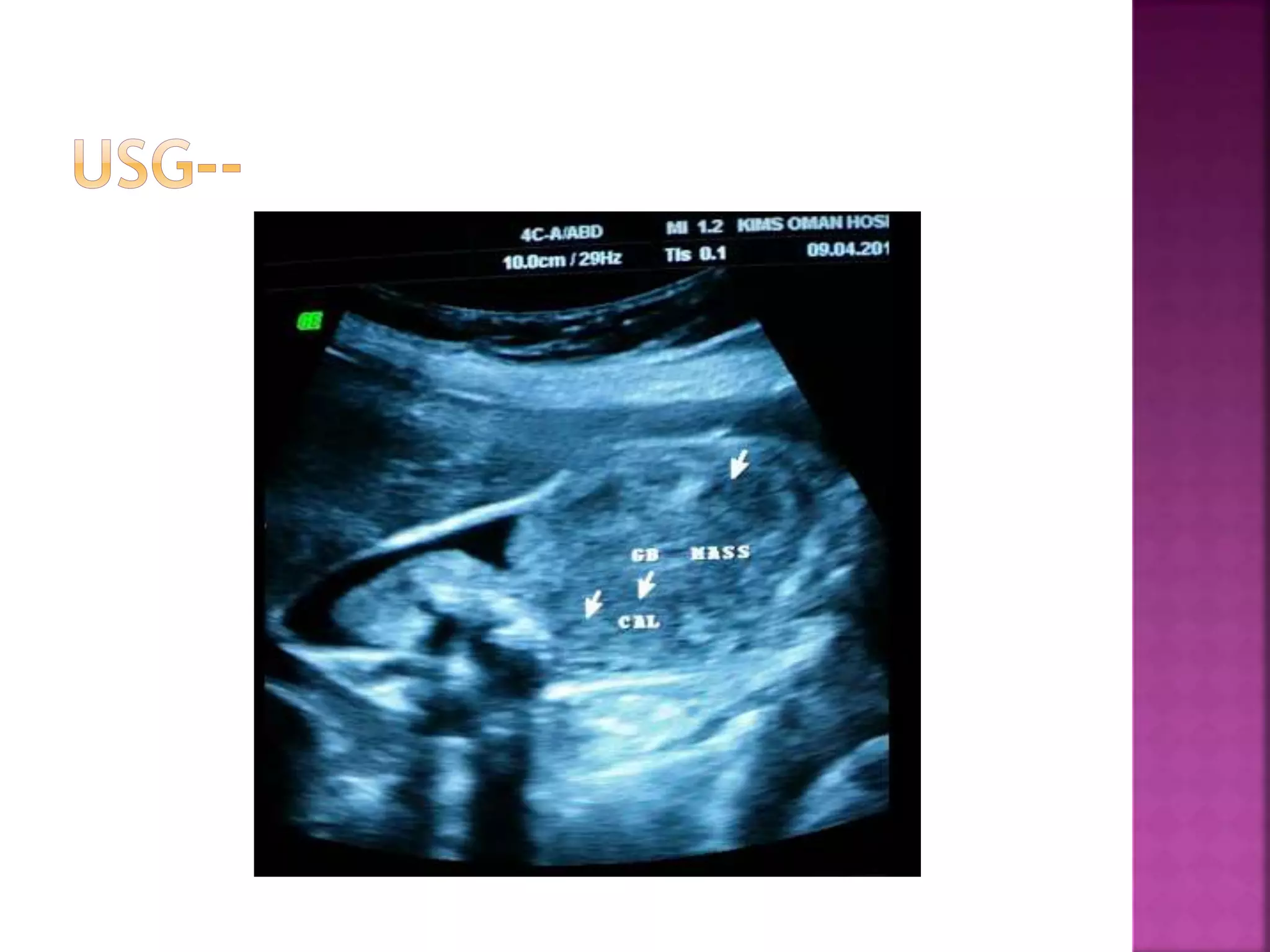
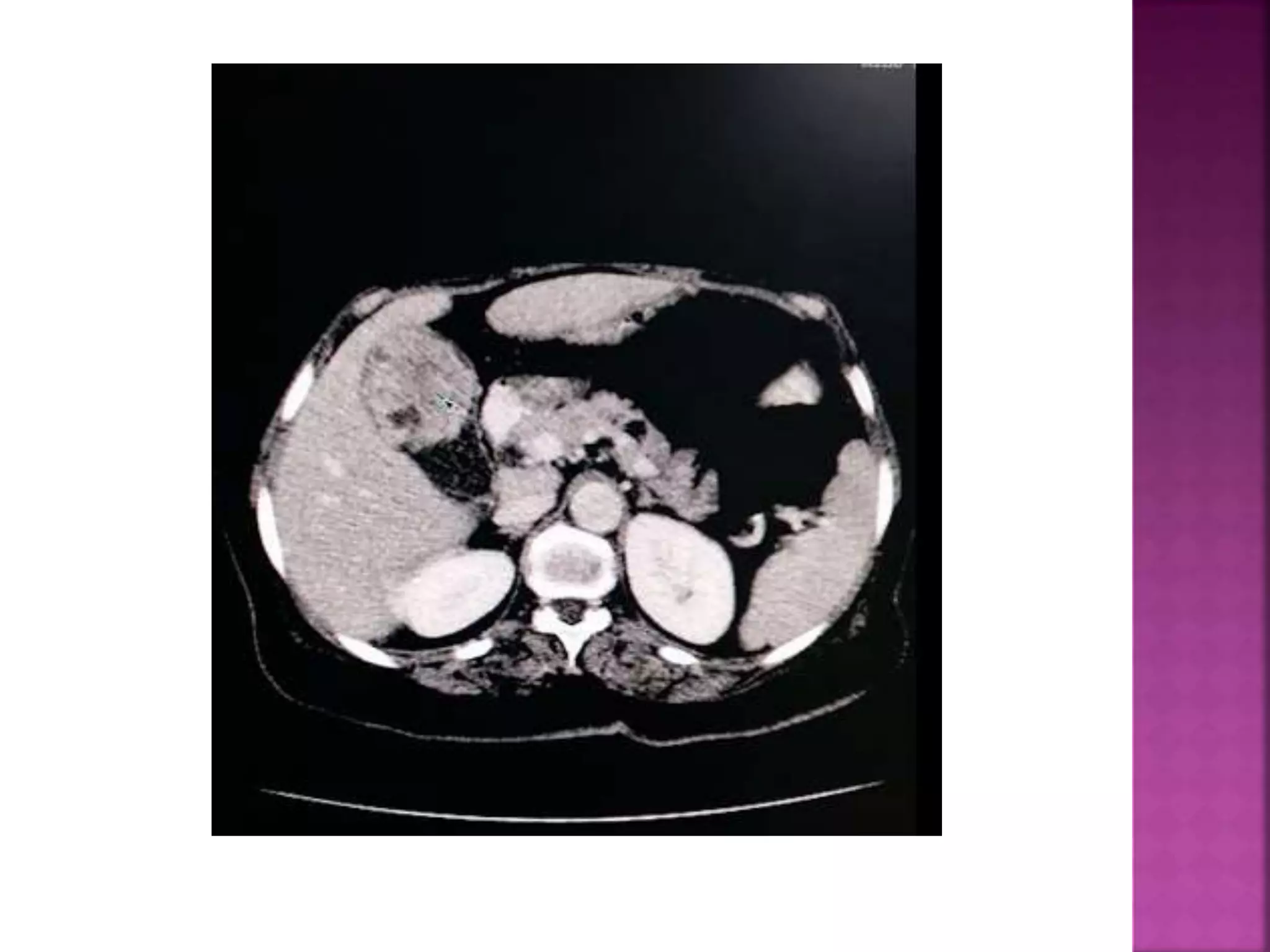
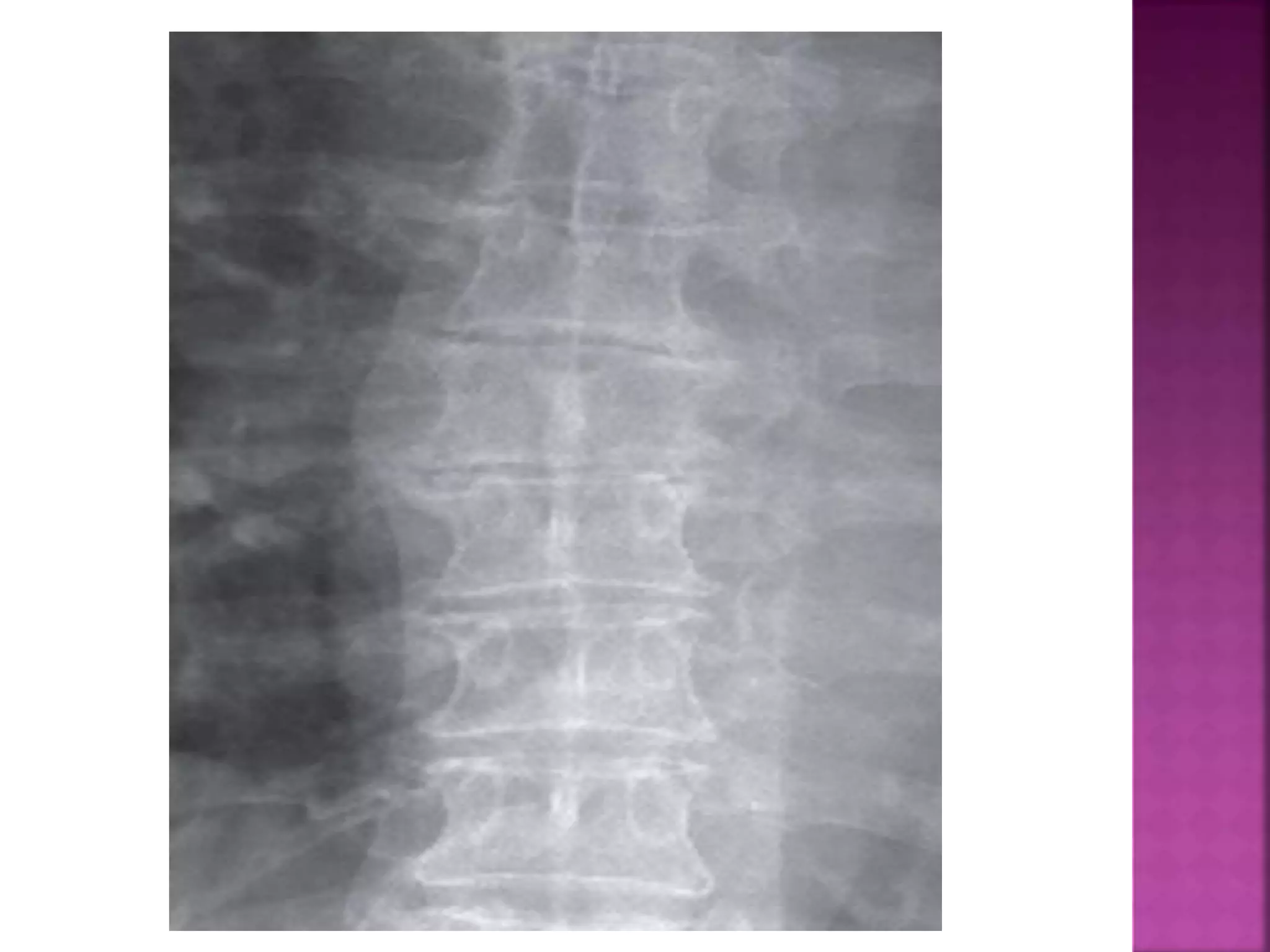
































































































The document discusses several radiology cases presented by Dr. Santhosh. It includes summaries of individual cases involving findings such as: 1) A gallbladder mass with local invasion and metastatic lesions in an abdominal imaging case. 2) Lucency seen over the liver on an abdominal x-ray of a renal transplant patient, which was later found to be biliary necrosis and abscess on CT scan. 3) Exercise-induced upper extremity deep vein thrombosis in 6 adolescent patients seen at a single center, who experienced poor outcomes with anticoagulation alone. 4) Additional cases involve findings such as diverticulitis, vein of Galen malformation, dandy walker cyst, and renal



































































