Download to read offline


![Introduction
• Slipped Capital Femoral Epiphysis (SCFE) incidence is
0.2 to 10 per 100.000. [Lehmann et al, 2006]
• Clinically, it can be classified into acute ,chronic, and
acute on top of chronic based on symptoms
duration. [Loder et al, 1993]
• Loder et al classified it into stable and unstable
based on the ambulatory status which predicts the
avascular necrosis (AVN) risk. [Loder et al, 1993]
• Radiologically, Southwick used his angle in lateral
view to place the slip into mild (< 300), moderate
(30-500), and severe (>500). [Southwick, 1973]](https://image.slidesharecdn.com/e4ts4riosbgmhusgqem8-signature-4e22566ff3720cbec963c1a4f0885a73e5c642e58ef42c3f1f3449b974bd3a51-poli-191023215951/75/Short-term-outcomes-of-Intertrochanteric-Imhauser-Osteotomy-combined-with-osteochondroplasty-in-slipped-capital-femoral-epiphysis-3-2048.jpg)



![•History [pain and function].
•Examination.
•Functional outcomes scores [HHS and WOMAC scores].
•Radiological Imaging [plain x ray and CT].
•Laboratory investigations:
Serum Ca, Po4, and alkaline phosphatase, serum vitamin
D level, thyroid profile, and routine preoperative labs.
Preoperative Evaluation](https://image.slidesharecdn.com/e4ts4riosbgmhusgqem8-signature-4e22566ff3720cbec963c1a4f0885a73e5c642e58ef42c3f1f3449b974bd3a51-poli-191023215951/75/Short-term-outcomes-of-Intertrochanteric-Imhauser-Osteotomy-combined-with-osteochondroplasty-in-slipped-capital-femoral-epiphysis-11-2048.jpg)
































![• Risk of implant failure (fixing thin cortical shell of epiphysis).
• Considerable risk of reoperation surgeries (for AVN, implant
failure, and hip dislocation): 18% in Upasani et al study.
• 40% of the cases were unstable cases which reflected the
focus of utilization of this technique in the unstable type.
• The most important indication for modified Dunn procedure
is unstable SCFE [Ziebarth et al, 2009]
Modified Dunn Procedure](https://image.slidesharecdn.com/e4ts4riosbgmhusgqem8-signature-4e22566ff3720cbec963c1a4f0885a73e5c642e58ef42c3f1f3449b974bd3a51-poli-191023215951/75/Short-term-outcomes-of-Intertrochanteric-Imhauser-Osteotomy-combined-with-osteochondroplasty-in-slipped-capital-femoral-epiphysis-49-2048.jpg)
![Based on the above, two institutes have modified their practice
patterns regarding modified Dunn procedure use in SCFE treatment:
Boston Children Hospital recommendations [Upasani et al, 2014]:
• A high-volume surgeon must be present during each modified Dunn
procedure.
• Restricted to acute severe unstable slippage within 24 hours of the
slippage to provide satisfactory results.
Javier et al recommendations: [Javier et al, 2017]
• The use of modified Dunn procedure in unstable SCFE was
abandoned in preference to gentle reduction, open capsulotomy,
and in situ pinning within 24 hours (lower AVN risk).
• Restricted its use to very selective stable severe cases with open
physis.
• It is better to choose another option as proximal femoral osteotomy
in concomitant with in situ pinning and osteochondroplasty.](https://image.slidesharecdn.com/e4ts4riosbgmhusgqem8-signature-4e22566ff3720cbec963c1a4f0885a73e5c642e58ef42c3f1f3449b974bd3a51-poli-191023215951/75/Short-term-outcomes-of-Intertrochanteric-Imhauser-Osteotomy-combined-with-osteochondroplasty-in-slipped-capital-femoral-epiphysis-50-2048.jpg)

































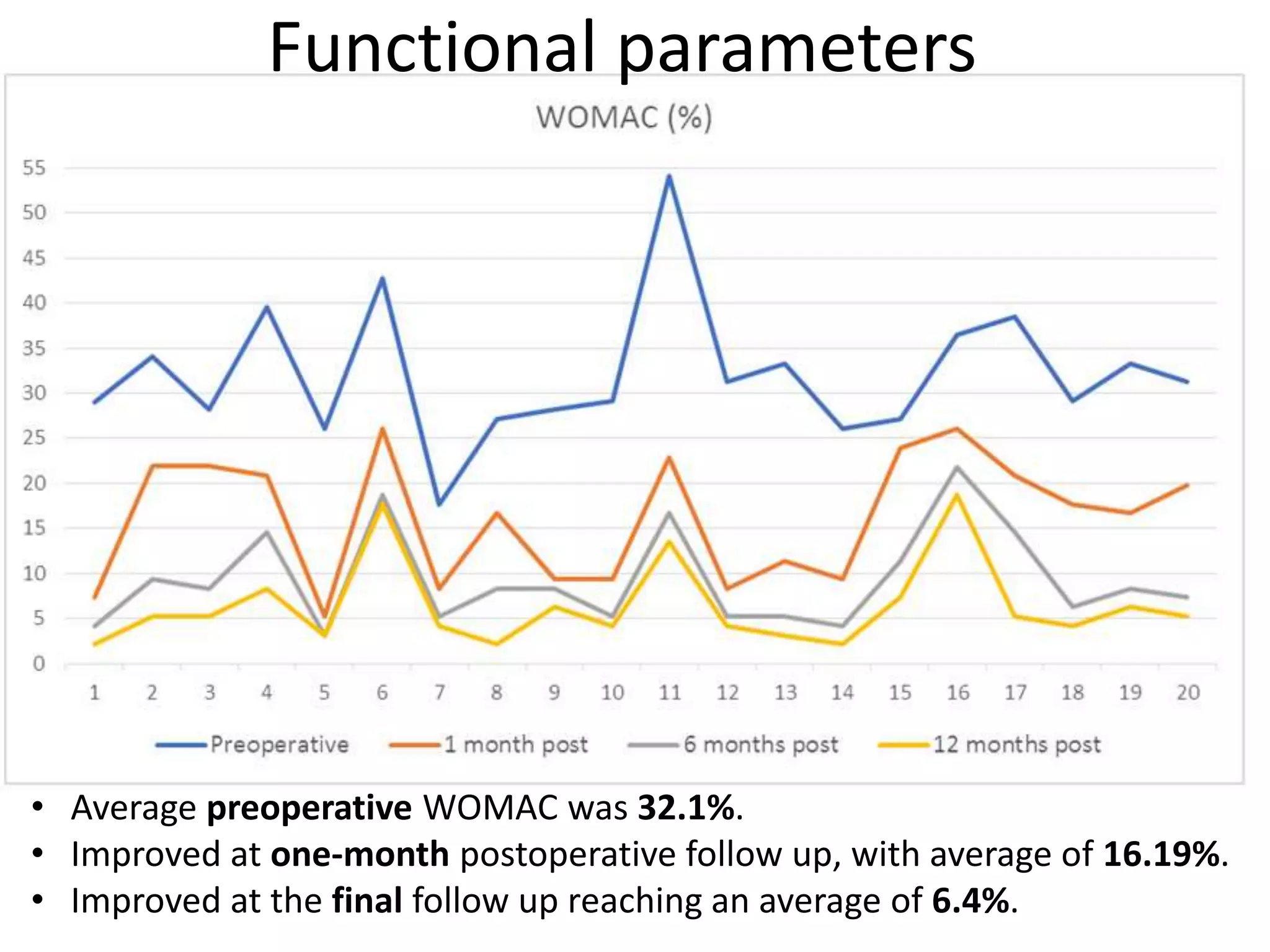
The document summarizes a study assessing the short-term outcomes of using intertrochanteric osteotomy combined with osteochondroplasty to treat moderate to severe stable slipped capital femoral epiphysis (SCFE). 20 hips were treated and followed for 12-24 months. Clinical and radiological outcomes improved significantly, with no cases of avascular necrosis or osteoarthritis. The approach was found to provide comparable results to modified Dunn procedure but without the risks of complications like avascular necrosis. It was concluded to be a preferred option for treating chronic stable moderate-severe SCFE.