Downloaded 30 times





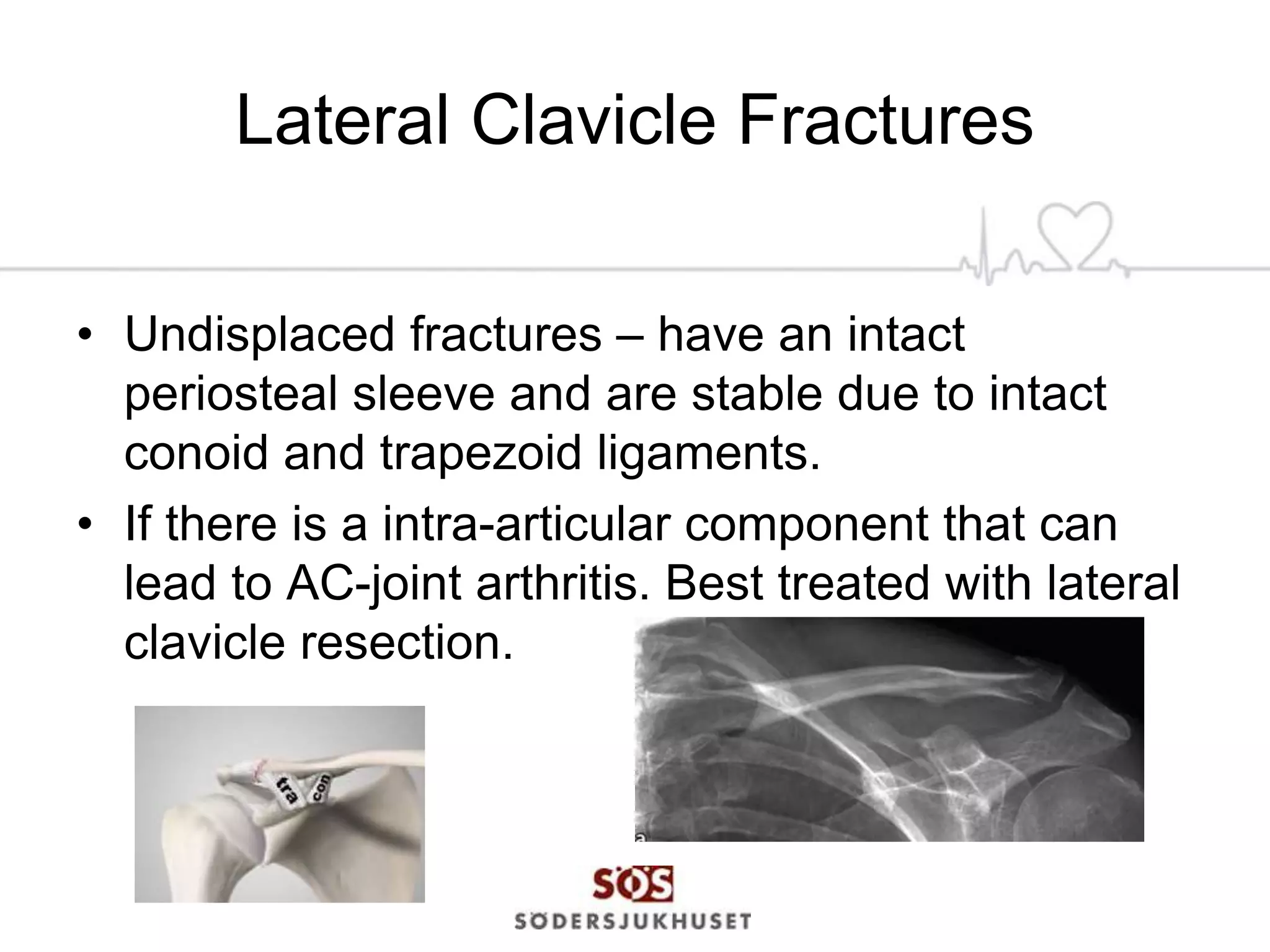














This document discusses classifications and treatments for clavicle fractures. It notes that midshaft fractures make up 80% of clavicle fractures. For midshaft fractures, displaced fractures may be treated surgically or non-surgically. A Cochrane review found no difference in outcomes between surgery and conservative treatment, though some studies found surgery resulted in fewer non-unions but more complications. The document concludes that treatment should be individualized based on the patient and fracture characteristics.


























![46 current evidence about femoral neck fracture treatment[1]](https://cdn.slidesharecdn.com/ss_thumbnails/46currentevidenceaboutfemoralneckfracturetreatment1-130613033628-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)